I’m going to add to that list today, but first let’s refresh our understanding of how government-caused “third-party payer” makes America’s health care system very expensive and inefficient.
The key insight is that consumers have little incentive to be smart shoppers when they perceive that other people are paying the bill. And health providers, needless to say, have little incentive to control costs when they know consumers care very little about prices.
Is this a big problem?
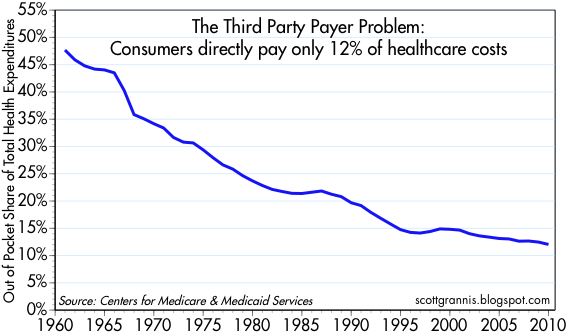
No, it is not a big problem. It is a giant problem. Here’s a chart, based on the federal government’s data, showing the share of health expenditures that are paid directly by consumers.
In the chart, I show the year that Obamacare was enacted. Notice that the legislation didn’t have an effect on the trendline, either the year it was enacted or in subsequent years as it was implemented.
And since Obamacare didn’t reduce the problem of third-party payer, one might guess that it didn’t solve the problem of rising health expenditures.
That guess would be correct, as shown in this column by Megan McArdle, which includes a predictably unsurprising headline.
…in 2022, the United States spent 16.6 percent of its gross domestic product on health care, while the next-highest spender, Germany, spent only 12.7 percent… As the Affordable Care Act took shape almost 15 years ago, its architects started looking for…savings… All these years later, we still haven’t found the magic money pot. …Obamacare contained a lot of elements that were expected to realize significant cost savings while actually improving the quality of care. …What this demonstrates is how hard it is to actually change the system in ways that generate major savings. …the wonks hunting for magic pots of money have mostly turned out to be chasing rainbows.
When I followed public policy in my younger days, I periodically would see stories about legislation that was approved by the House of Representatives with only one dissenting vote.
My memory isn’t perfect, I’m sure, but it seems that Ron Paul was always that lonely member. And my recollection is that he was (as usual) always on the correct side, voting for liberty and against government.
Something similar happened yesterday, except this time six members of Congress voted against a repeal of the “Cadillac Tax” that is part of Obamacare.
It was an eclectic group, but it included Justin Amash and Chip Roy, who are two of the most committed and principled supporters of free markets and limited government in Congress.
From the right, I recommend this analysis from Alan Viard at the American Enterprise Institute.
…employer-provided health insurance gets a big tax break. Workers pay income and payroll taxes on their cash wages, but not on their health insurance benefits. …the tax break is poorly targeted because it applies even to high-cost “Cadillac” health plans. The tax system should not artificially encourage Cadillac plans, which boost demand for medical services and drive up health care costs for everyone. Although the Cadillac tax does not directly change the tax break for high-cost employer plans, it offsets the break by imposing a separate 40 percent tax on those plans. That round-about approach is far from ideal, but it gets the job done. …the Cadillac tax has won support from economists across the ideological spectrum.
From the left, here’s some of what Bruce Bartlett wrote for the New York Times.
Although obviously a form of income to the worker, the Internal Revenue Service nevertheless ruled that it was not taxable, although businesses could still deduct the cost. This anomalous tax treatment was a fabulous tax loophole for both businesses and workers… Congress codified the I.R.S. ruling.. Various tax expenditures for health cost hundreds of billions of dollars in lost revenue per year, according to the Congressional Research Service. Eliminating them could finance a significant reduction in tax rates. …If the Republicans are serious about using tax reform to improve the competitiveness of American businesses, the best thing they can do is reform employer-based health insurance.
For honest folks on the left, they should be motivated by the fact that this exclusion overwhelmingly benefits upper-income taxpayers.
I very much suspect Obama partisans and Trump partisans won’t like this column, but the sad reality is that both Obamacare and Trump’s protectionism have a lot in common.
In both cases, government is limiting the freedom of buyers and sellers to engage in unfettered exchange.
In both cases, the fiscal burden of government increases.
In both cases, politicians misuse statistics to expand the size and scope of government.
Today, let’s add another item to that list.
In both cases, the Washington swamp wins thanks to increased cronyism and corruption.
To see what I mean, let’s travel back in time to 2011. I wrote a column about Obamacare and cited some very persuasive arguments by Tim Carney that government-run healthcare (or, to be more accurate, expanded government control of healthcare) was creating a feeding frenzy for additional sleaze in Washington.
Congress imposes mandates on other entities, but gives bureaucrats the power to waive those mandates. To get such a waiver, you hire the people who used to administer or who helped craft the policies. So who’s the net winner? The politicians and bureaucrats who craft policies and wield power, because this combination of massive government power and wide bureaucratic discretion creates huge demand for revolving-door lobbyists.
I then pointed out that the sordid process of Obamacare waivers was eerily similar to a passage in Atlas Shrugged.
Wesley Mouch…issued another directive, which ruled that people could get their bonds “defrozen” upon a plea of “essential need”: the government would purchase the bonds, if it found proof of the need satisfactory. …One was not supposed to speak about the men who…possessed needs which, miraculously, made thirty-three frozen cents melt into a whole dollar, or about a new profession practiced by bright young boys just out of college, who called themselves “defreezers” and offered their services “to help you draft your application in the proper modern terms.” The boys had friends in Washington.
Well, the same thing is happening again. Only this time, as reported by the New York Times, protectionism is the policy that is creating opportunities for swamp creatures to line their pockets.
The Trump administration granted seven companies the first set of exclusions from its metal tariffs this week and rejected requests from 11 other companies, as the Commerce Department began slowly responding to the 20,000 applications that companies have filed for individual products. …several companies whose applications were denied faced objections from American steel makers. …companies that have applied for the exclusions criticized the exercise as both long and disorganized. “This is the most screwed-up process,” said Mark Mullen, president of Griggs Steel, a steel distributor in the Detroit area. “This is a disservice to our industry and the biggest insult to our intelligence that I have ever seen from the government.”
From an economic perspective, it certainly is true that this new system is “disorganized” and “a disservice” and an “insult to our intelligence.” Those same words could be used to describe the welfare state, the EEOC, farm subsidies, the tax code, and just about everything else the government does.
But there’s one group of people who are laughing all the way to the bank, The lobbyists, consultants, fixers, and other denizens of the swamp are getting rich. Whether they’re preparing the applications, lobbying for the applications, or lobbying against the applications, they are getting big paychecks.
And the longer this sordid protectionist process continues, we will see a repeat of what happened with Obamacare as senior-level people in government move through the revolving door so they can get lucrative contracts to help clients manipulate the system (yes, Republicans can be just as sleazy as Democrats).
First, it is very bureaucratic and inefficient to use insurance for routine medical expenses. Sort of like using auto insurance to cover the cost of getting an oil change.
Second, insurance coverage means third-party payer, which means birth control will become more expensive(albeit financed by premiums rather than out of pocket).
Fifth, if politicians and bureaucrats really want birth control to be more affordable, they would make the pill available over the counter instead of requiring a prescription.
President Trump recently announced that his Administration would relax the mandate. I think that is good news for the above reasons.
Critics are very upset. But rather than argue about the desirability of insurance coverage and the wisdom of Washington mandates, they’re actually claiming that the White House has launched some sort of war on birth control. I’m not joking.
Jeff Jacoby of the Boston Globeanalyzes the issue. He starts by observing that nobody is proposing to ban birth control
…the Supreme Court ruled, in Griswold v. Connecticut, that government may not ban anyone from using contraceptives. …That freedom is a matter of settled law, and hasn’t been challenged in the slightest by President Trump or his administration.
He then points out that some folks on the left have gone ballistic.
Hillary Clinton accused Trump of showing “blatant disregard for medicine, science, & every woman’s right to make her own health decisions.” Elizabeth Warren, denouncing “this attack on basic health care,” claimed that the GOP’s top priority is to deprive women of birth control.
Their arguments, however, are utter nonsense. If Person A no longer has to subsidize Person B, that doesn’t mean Person B can’t buy things. It simply means there won’t be third-party payer.
Jacoby agrees.
News flash to Warren, et al.: There is no attack on health care, and no in America is being deprived of birth control. You are losing nothing but the power to force nuns to pay for your oral contraceptives. …As a matter of economics and public policy, the Affordable Care Act mandate that birth control be supplied for free is absurd. …Especially since birth control will remain as available and affordable as ever.
Indeed, the Trump Administration was actually far too timid. There should be no birth-control mandate for any insurance plan. It should be something negotiated by employers and employees.
…the new White House rule leaves the birth-control mandate in place. Trump’s “tweak won’t affect 99.9 percent of women,” observes the Wall Street Journal, “and that number could probably have a few more 9s at the end.” Washington will continue to compel virtually every employer and insurer in America to supply birth control to any woman who wants one at no out-of-pocket cost.
Jacoby closes his column with some very sensible observations and recommendations.
…there is no legitimate rationale for such a mandate. Americans don’t expect to get aspirin, bandages, or cold medicine — or condoms — for free; by what logic should birth control pills or diaphragms be handed over at no cost? …By and large, birth control is inexpensive; as little as $20 a month without insurance. …access to birth control, as the Centers for Disease Control reported in 2010, was virtually universal before Obamacare. The White House is right to end the burden on religious objectors. But it is the birth-control mandate itself that should be scrapped. Contraception is legal, cheap, and available everywhere. Why are the feds meddling where they aren’t needed?
The last sentence is key. The federal government (heck, no level of government) should be involved with birth control. They shouldn’t ban it. And they shouldn’t mandate it, either.
P.S. About five years ago, Sandra Fluke got her 15 minutes of fame by asserting that she had a right to third-party-financed birth control. That led to some clever jokes, including this cartoon and this video.
For what it’s worth, I think this cartoon is the best summary of the issue.
P.P.S. Predictably, the United Nations supports a “right” to taxpayer-financed birth control.
In the eight years of writing this column, I’ve periodically confessed to certain fantasies. But you’ll notice that these fantasies don’t involve supermodels from Victoria’s Secret (though they did make a cameo appearance in one column).
Instead, either because I’m getting old or because I’m a dorky libertarian, my fantasies involve public policy. Here are imaginary things that have caused my pulse to quicken.
Trump…can restore the Constitution’s limits on executive power, provide relief to Americans suffering under Obamacare, and hasten repeal.
Michael has a 14-point list, but here are the ones that matter for our purposes today.
First, put pressure on Congress.
1. End Congress’s illegal Obamacare exemption. Obamacare threw members of Congress and congressional staff out of their health plans and in effect cut their pay by up to $12,000 per year. Obama ignored the law and made illegal payments to private insurance companies on behalf of members of Congress and their staff for six years — all to prevent Congress from reopening the law. Trump should announce that he will end those illegal payments immediately, and that he will veto any bill restoring the pay cut that Obamacare dealt Congress, until Congress earns that money by repealing and replacing the law. Congress shouldn’t get an exemption from Obamacare until the American people do. Democrats who actually voted for Obamacare especially should have to live under it.
Second, put pressure on insurance companies.
2. End Obamacare’s unconstitutional cost-sharing subsidies. In House v. Burwell, a federal judge ruled that the Obama administration “violate[d] the Constitution” by paying billions of dollars in “cost-sharing” subsidies to private insurance companies without a congressional appropriation. Trump should immediately drop the Obama administration’s appeal of that decision, stop the unconstitutional payments, and prevent insurers from canceling Obamacare plans until 2018.
3. End Obamacare’s illegal “reinsurance” payments. The Government Accountability Office found that the Obama administration illegally diverted additional billions of dollars in “reinsurance” payments from the Treasury to private insurance companies. Trump should immediately stop the diversion of those funds and demand that insurers repay the more than $3 billion in unlawful payments they have received.
4. Block Big Insurance’s “risk-corridor” raid on the Treasury. The Obama administration tried to circumvent a statutory cap on “risk-corridor” payments to private insurance companies by offering to settle lawsuits filed by the insurers. Trump should immediately announce that his administration will not settle but will instead vigorously defend taxpayers’ interests in all such lawsuits.
Needless to say, the combination of angst-ridden folks on Capitol Hill and angst-ridden bigwigs from insurance companies would probably be more than enough to get weak-kneed Republicans to climb on board for repeal.
Indeed, in my fantasy, Trump uses his bully pulpit (and Twitter account) to specifically pressure those callow Republicans who voted for major repeal in 2015 and then flip-flopped and voted against various (usually partial) repeal proposals earlier this month.
Various media sources certainly agree that Trump has a huge amount of leverage.
Ending the CSR subsidies, paid monthly to insurers, is one way that Trump could hasten Obamacare’s demise without legislation, by prompting more companies to raise premiums in the individual market or stop offering coverage. …health-care analyst Spencer Perlman at Veda Partners LLC said in a research note that there’s a 30 percent chance Trump will end CSR payments, which may “immediately destabilize the exchanges, perhaps fatally.” …Many insurers have already dropped out of Obamacare markets in the face of mounting losses, and blamed the uncertainty over the future of the cost-sharing subsidies and the individual mandate as one of the reasons behind this year’s premium increases.
President Donald Trump announced on Saturday that if Congress doesn’t act soon on health care, he could end federal “BAILOUTS” for insurance companies, which could effectively force Congress to act or else put health insurance companies in the difficult position of having to raise rates on people who can’t afford to pay them or to leave Obamacare exchanges entirely. …The “BAILOUTS” to insurance companies Trump referred to in his tweet are “cost sharing reduction” payments… If Trump were to withhold these funds from health insurance companies, it would likely result in many insurers choosing to leave the Obamacare health insurance exchanges… If health insurance companies choose to leave the insurance exchanges, which is the most likely response, it could catalyze the collapse of the Obamacare exchange system, making it more difficult for members of Congress to wait on implementing a repeal and replace bill.
And here are passages from a Wall Street Journalstory.
President Donald Trump made one of his most explicit threats to cut off payments to insurance companies to force senators and lobbyists back to the bargaining table for a GOP health-care bill, and saying, for the first time, that he was also willing to cancel some of lawmakers’ health-care benefits. …Those payments have been challenged in court by House Republicans, who argue the funds were never authorized by Congress. A federal judge has sided with the House but allowed the payments to continue until the litigation concludes. Democrats have said that cutting off the payments would be tantamount to sabotaging the insurance markets… Mr. Trump’s Saturday tweet…also the first to mention that he was open to another idea proposed by conservative activists to pull lawmakers back to the task of a health-care bill: cutting off their existing health benefits. …some lawmakers contending that it is an end-run around a provision in the 2010 health law that requires members of Congress to get their health coverage like other Americans.
Keep in mind, by the way, that this isn’t just a matter of political brinksmanship. The various payments to insurance companies are either not authorized by the law, or they were authorized and Congress has declined to appropriate funds. In other words, these payments make a mockery of the rule of law. They are illegal and/or unconstitutional.
Moreover, my former Heritage colleague Mike Needham has a good explanation of how the Obama Administration preposterously decided to classify Congress as a small business in order to enable subsidies that were not part of the Obamacare legislation. Once again, throwing the rule of law overboard for political convenience (which was a pattern with the previous Administration).
So even if Trump didn’t want to get rid of Obamacare, these payments should end.
But we may as well make a policy virtue out of legal necessity by getting rid of these payments as part of a campaign to pressure Capitol Hill to do what’s right and get rid of the disastrous Obamacare legislation.
P.P.S. From the moment he emerged on the national stage, I’ve been worried that Donald Trump would preside over an expansion in the burden of government. But if there’s a libertarian bone in his body, it becomes apparent when he tweets. Not only did he tweet a very appropriate and effective threat against Obamacare yesterday, he also tweeted a very appropriate and effective threat about a government shutdown back in May.
P.P.S. It wasn’t one of my fantasies, but here’s something from 2013 about a libertarian fantasy dealing with ammo and sex.
Senate Republicans have produced their Obamacare repeal legislation, though as I noted at the end of this interview, it’s really more a bill about Medicaid reform than Obamacare repeal.
But critics are savaging this idea, implying that “deep cuts” will hurt the quality of care. Indeed, some of them are even engaging in poisonous rhetoric about people dying because of cutbacks.
There’s one small problem with the argument, however. Nobody is proposing to cut Medicaid. Republicans are merely proposing to limit annual spending increases. Yet this counts as a “cut” in the upside-down world of Washington budgeting.
The Washington Post contributes to innumeracy with a column explicitly designed to argue that the program is being cut.
…the Senate proposal includes significant cuts to Medicaid spending…the Senate bill is more reliant on Medicaid cuts than even the House bill…spending on the program would decline in 2026 by 26 percent…That’s a decrease of over $770 billion on Medicaid over the next 10 years. …By 2026, the federal government would cut 1 of every 4 dollars it spends on Medicaid.
An article in the New York Times has a remarkably inaccurate headline, which presumably isn’t the fault of reporters. Though the story has its share of dishonest rhetoric, especially in the first few paragraphs.
Senate Republicans…took a major step…, unveiling a bill to make deep cuts in Medicaid… The Senate measure…would also slice billions of dollars from Medicaid, a program that serves one in five Americans… The Senate bill would also cap overall federal spending on Medicaid: States would receive a per-beneficiary allotment of money. …State officials and health policy experts predict that many people would be dropped from Medicaid because states would not fill the fiscal hole left by the loss of federal money.
“Loss of federal money”?
I’d like to lose some money using that math. Here’s a chart showing the truth. The data come directly from the Congressional Budget Office.
At the risk of pointing out the obvious, it’s not a cut if spending rises from $393 billion to $464 billion.
Federal outlays on the program will climb by about 2 percent annually.
By the way, it’s perfectly fair for opponents to say that they want the program to grow faster in order to achieve different goals.
But they should be honest with numbers.
Now that we’ve addressed math, let’s close with a bit of policy.
The Wall Street Journal recently opined on the important goal of giving state policymakers the power and responsibility to manage the program. The bottom line is that recent waivers have been highly successful.
…center-right and even liberal states have spent more than a decade improving a program originally meant for poor women and children and the disabled. Even as ObamaCare changed Medicaid and exploded enrollment, these reforms are working… The modern era of Medicaid reform began in 2007, when Governor Mitch Daniels signed the Healthy Indiana Plan that introduced consumer-directed insurance options, including Health Savings Accounts (HSAs). Two years later, Rhode Island Governor Donald Carcieri applied for a Medicaid block grant that gives states a fixed sum of money in return for Washington’s regulatory forbearance. Both programs were designed to improve the incentives to manage costs and increase upward mobility so fewer people need Medicaid. Over the first three years, the Rhode Island waiver saved some $100 million in local funds and overall spending fell about $3 billion below the $12 billion cap. The fixed federal spending limit encouraged the state to innovate, such as reducing hospital admissions for chronic diseases or transitioning the frail elderly to community care from nursing homes. The waiver has continued to pay dividends under Democratic Governor Gina Raimondo. …This reform honor roll could continue: the 21 states that have moved more than 75% of all beneficiaries to managed care, Colorado’s pediatric “medical homes” program, Texas’s Medicaid waiver to devolve control to localities from the Austin bureaucracy.
By contrast, the current system is not successful.
Avik Roy explained this perverse result in Forbes back in 2013.
Piles of studies have shown that people on Medicaid have health outcomes that are no better, and often worse, than those with no insurance at all. …authors of the Oregon study published their updated, two-year results, finding that Medicaid “generated no significant improvement in measured physical health outcomes.” The result calls into question the $450 billion a year we spend on Medicaid… And all of that, despite the fact that the study had many biasing factors working in Medicaid’s favor: most notably, the fact that Oregon’s Medicaid program pays doctors better; and also that the Medicaid enrollees were sicker, and therefore more likely to benefit from medical care than the control arm.
In other words, I was understating things when I wrote above that there was “one small problem” with the left’s assertion about Medicaid cuts hurting people.
Yes, the fact that there are no actual cuts is a problem with that argument. But the second problem with the left’s argument is that Medicaid doesn’t seem to have any effect on health outcomes. So if Republicans actually did cut the program, it’s unclear how anybody would suffer (other than the fraudsters who bilk the program).
Back in 2015, I basically applauded the Congressional Budget Office for its analysis of what would happen if Obamacare was repealed. The agency’s number crunchers didn’t get it exactly right, but they actually took important steps and produced numbers showing how the law was hurting taxpayers and the economy.
Now we have a new set of Obamacare numbers from CBO based on the partial repeal bill approved by the House of Representatives. The good news is that the bureaucrats show substantial fiscal benefits. There would be a significant reduction in the burden of spending and taxation.
But the CBO did not show very favorable numbers in other areas, most notably when it said that 23 million additional people would be uninsured if the legislation was enacted.
Part of the problem is that Republicans aren’t actually repealing Obamacare. Many of the regulations that drive up the cost of health insurance are left in place.
My colleague at Cato, Michael Cannon, explains why this is a big mistake.
Rather than do what their supporters sent them to Washington to do – repeal ObamaCare and replace it with free-market reforms – House Republicans are pushing a bill that will increase health-insurance premiums, make health insurance worse for the sick… ObamaCare’s core provisions are the “community rating” price controls and other regulations that (supposedly) end discrimination against patients with preexisting conditions. …Community rating is the reason former president Bill Clinton called ObamaCare “the craziest thing in the world” where Americans “wind up with their premiums doubled and their coverage cut in half.” Community rating is why women age 55 to 64 have seen the highest premium increases under ObamaCare. It is the principal reason ObamaCare has caused overall premiums to double in just four years. Community rating literally penalizes quality coverage for the sick… ObamaCare is community rating. The AHCA does not repeal community rating. Therefore, the AHCA does not repeal ObamaCare.
It would be ideal if Republicans fully repealed Obamacare.
But maybe that’s hoping for too much since many Republicans are squeamish about supporting even a watered-down proposal to modify Obamacare.
That being said, there are some reasonable complaints that CBO overstated the impact of the GOP bill.
Doug Badger and Grace Marie Turner, for instance, were not impressed by CBO’s methodology.
The Congressional Budget Office (CBO) launched its latest mistaken Obamacare-related estimate this week, predicting that a House-passed bill to repeal and replace the embattled law would lead to 23 million more uninsured people by 2026. …the agency’s errors are not only massive – one of their predictions of 2016 exchange-based enrollment missed by 140%… Undaunted by failure and unschooled by experience, CBO soldiers on, fearlessly predicting that millions will flock to the exchanges any day now. …CBO measures the House-passed bill against this imaginary baseline and finds it wanting. …One reason CBO gets it so wrong so consistently is its fervent belief that the individual mandate has motivated millions to enroll in coverage. …CBO’s belief in the power of the individual mandate is misplaced. …The IRS reports that in the 2015 tax year, 6.5 million uninsured filers paid the tax penalty, 12.7 million got an exemption and additional 4.2 million people simply ignored the penalty. They left line 61 on their form 1040 blank, refusing to tell the government whether or not they had insurance. …In all, that is a total of 23.4 million uninsured people – out of an estimated 28.8 million uninsured – who either paid, avoided or ignored the penalty. That hardly suggests that the mandate has worked.
The Wall Street Journal also was quite critical of the CBO analysis.
…the budget scorekeepers claim the House bill could degrade the quality of insurance. This editorializing could use some scrutiny. Without government supervision of insurance minutiae and a mandate to buy coverage or pay a penalty, CBO asserts, “a few million” people will turn to insurance that falls short of the “widely accepted definition” of “a comprehensive major medical policy.” They might select certain forms of coverage that Obama Care banned, like “mini-med” plans with low costs and low benefits. Or they might select indemnity plans that pay a fixed-dollar amount per day for illness or hospitalization, or dental-only or vision-only single-service plans. CBO decided to classify these people as “uninsured,” though without identifying who accepts ObamaCare’s definition of standardized health benefits and why they deserve to substitute their judgment for the choices of individual consumers. …But the strangest part of CBO’s preoccupation with “high-cost medical events” is that the analysts never once mention catastrophic coverage—not once. These types of plans didn’t cover routine medical expenses but they did protect consumers against, well, a high-cost medical event like an accident or the diagnosis of a serious illness. Those plans answered what most people want most out of insurance—financial security and a guarantee that they won’t be bankrupted by cancer or a distracted bus driver. …under the House reform Americans won’t have any problem insuring against a bad health event, even if CBO won’t admit it. …CBO has become a fear factory because it prefers having government decide for everybody.
Drawing on his first-hand knowledge, Dr. Marc Siegel wrote on the issue for Fox News.
…23 million…will lose their health insurance by 2026 if the American Health Care Act, the bill the House passed to replace ObamaCare, is passed in the Senate and signed by President Trump. This number is concerning — until you look at it and the CBO’s handling of the health care bills more closely. …First, the CBO was wildly inaccurate when it came to ObamaCare, predicting that 23 million people would be getting policies via the exchanges by 2016. The actual number ended up being only 10.4 million… Second, many who chose to buy insurance on the exchanges did so only because they wanted to avoid paying the penalty, not because they needed or wanted the insurance. Many didn’t buy insurance until they got sick.
IN the real world, people who don’t have insurance coverage cannot lose it. Yet…the CBO estimates 14 million fewer people will have coverage in 2018 if the House bill is enacted than would be the case if the ACA is left intact, and 23 million fewer by 2026. …In 2016, there were roughly 10 million people obtaining insurance through an Obamacare exchange. The CBO estimated that number would suddenly surge to 18 million by 2018 if the law was left intact, but that far fewer people would be covered if the House reforms became law. Put simply, the CBO estimated that millions of people who don’t have insurance through an exchange today would “lose” coverage they would otherwise obtain next year. That’s doubtful. …At one point, the office estimated 22 million people would receive insurance through an Obamacare exchange by 2016. As already noted, the actual figure was less than half that. One major reason for the CBO being so far off the mark is that federal forecasters believed Obamacare’s individual mandate would cause people to buy insurance, regardless of cost. That hasn’t proven true. …In a nutshell, the CBO predicts reform would cause millions to lose coverage they don’t now have, and that millions more would eagerly reject the coverage they do have because it’s such a bad deal. Those aren’t conclusions that bolster the case for Obamacare.
CBO says 14 million fewer people on net would be insured in 2018 relative to the ObamaCare status quo, rising to 23 million in 2026. The political left has defined this as “losing coverage.” But 14 million would roll off Medicaid as the program shifted to block grants, which is a mere 17% drop in enrollment after the ObamaCare expansion. The safety net would work better if it prioritized the poor and disabled with a somewhat lower number of able-bodied, working-age adults. The balance of beneficiaries “losing coverage” would not enroll in insurance, CBO says, “because the penalty for not having insurance would be eliminated.” In other words, without the threat of government to buy insurance or else pay a penalty, some people will conclude that ObamaCare coverage isn’t worth the price even with subsidies. …CBO’s projections about ObamaCare enrollment…were consistently too high and discredited by reality year after year. CBO is also generally wrong in the opposite direction about market-based reforms, such as the 2003 Medicare drug benefit whose costs the CBO badly overestimated.
Here are excerpts from Seth Chandler’s Forbescolumn.
My complaints about the CBO largely revolve around its dogged refusal to adjust its computations to the ever-more-apparent failings of the Affordable Care Act. When the CBO says that 23 million fewer people will have insurance coverage under the AHCA than under the ACA — a statistic that politics have converted into a mantra — that figure is predicated on an ACA that no longer exists. It is based on the continuing assumption that the ACA will have 18 million people enrolled on its exchanges in 2018 and that this situation will persist until 2026. I know no one on any side of the political spectrum who believes this to be true. The ACA has about 11 million people currently enrolled on its exchanges in 2017 and, with premiums going up, some insurers withdrawing from various markets, and the executive branch fuzzing up whether the individual mandate will actually be enforced. The consensus is that ACA enrollment will stay the same or go down, not increase 60%.
And here’s some of what Drew Gonshorowski wrote for the Daily Signal.
…reducing premium levels by rolling back regulations could actually have the effect of making plans more desirable for individuals looking to pay less. The CBO lacks any real discussion of these positive effects. …The CBO’s score on Medicaid…reflects that it assumes more states would likely have expanded in the future under the Affordable Care Act. Thus, its projection that 14 million fewer people would be insured due to not having Medicaid under the American Health Care Act might be overstated… CBO…assumes the Affordable Care Act will enroll 7 to 8 million more people in the individual market, when in reality it does not appear this will be the case
Last but not least, my former colleague Robert Moffit expressed concerns in a column for USA Today. The part that caught my eye was that CBO has a less-than-stellar track record on Obamacare projections.
The GOP should be skeptical of CBO’s coverage estimates. It has been an abysmal performance. For example, CBO projected initially that 21 million persons would enroll in exchange plans in 2016. The actual enrollment: 11.5 million.
The bottom line is that CBO overstated the benefits of Obamacare, at least as measured by the number of people who would sign up for the program.
The bureaucrats were way off.
Yet CBO continues to use those inaccurate numbers, creating a make-believe baseline that is then used to estimate a large number of uninsured people if the Republican bill is enacted.
P.S. You may be wondering why Republicans don’t fully repeal Obamacare so that they can get credit for falling premiums. Part of the problem is that they are using “reconciliation” legislation that supposedly is limited to fiscal matters. In other words, you can’t repeal red tape and regulation. At least according to some observers. I think that’s silly since such interventions drive up the cost of health care, which obviously has an impact on the budget. Also, Republicans are a bit squeamish about reducing subsidies for various groups, whether explicit (like the Medicaid expansion) or implicit (like community rating). In other words, the Second Theorem of Government applies.
For three decades, I’ve been trying to convince politicians to adopt good policy. I give them theoretical reasons why it’s a good idea to have limited government. I share with them empirical evidence demonstrating the superiority of free markets over statism. And I’m probably annoyingly relentless about disseminating examples of good and bad policy from around the world (my version of “teachable moments”).
But if you want to get a politician to do the right thing, you need more than theory, data, and real-world case studies. You need to convince them – notwithstanding my Second Theorem of Government – that good policy won’t threaten their reelection.
My usual approach is to remind them that Ronald Reagan adopted a bunch of supposedly unpopular policies, yet he got reelected in a landslide because reducing the burden of government allowed the private sector to grow much faster. George H.W. Bush, by contrast, became a one-term blunder because his tax increase and other statist policies undermined the economy’s performance.
I’m hoping this argument will resonate with some of my friends who are now working in the White House. And I don’t rely on vague hints. In this clip from a recent interview, I bluntly point out that good policy is good politics because a faster-growing economy presumably will have a big impact on the 2020 election.
But the Republican plan did not try to fix the government-imposed third-party-payer distortions that cause health care to be so expensive and inefficient. And I pointed out at the end of this clip that Republicans would have been held responsible as the system got even more costly and bureaucratic.
Now let’s shift to fiscal policy.
Here’s a clip from an interview about Trump’s budget. I’m happy about some of the specific reductions (see here, here, and here), but I grouse that there’s no attempt to fix entitlements and I’m also unhappy that the reductions in domestic discretionary spending are used to benefit the Pentagon rather than taxpayers.
The latter half of the above interview is about the corruption that defines the Washington swamp. Yes, it’s possible that Trump could use the “bully pulpit” to push Congress in the right direction, but I wish I had more time to emphasize that shrinking the overall size of government is the only way to really “drain the swamp.”
And since we’re talking about good policy and good politics, here’s a clip from another interview.
Back when the stock market was climbing, I suggested it was a rather risky move for Trump to say higher stock values were a referendum on the benefits of his policies. After all, what goes up can go down.
The hosts acknowledge that the stock market may decline in the short run, but they seem optimistic in the long run based on what happened during the Reagan years.
In other words, there was a direct connection between good policy, good economy, and good political results. Indeed, let’s enshrine this relationship in a “Fourth Theorem of Government.”
For what it’s worth, Reagan also demonstrated leadership, enacting all those pro-growth reforms over the vociferous opposition of various interest groups.
Will Trump’s reform be that bold and that brave? His proposed 15-percent corporate tax rate deserves praise, and he seems serious about restraining the regulatory state, but he will need to do a lot more if he wants to be the second coming of Ronald Reagan. Not only will he need more good policies, but he’ll also need to ditch some of the bad policies (childcare subsidies, infrastructure pork, carried-interest capital gains tax hike, etc) that would increase the burden of government.
The jury is still out, but I’m a bit pessimistic on the final verdict.
I’m flabbergasted when people assert that America’s costly and inefficient healthcare system is proof that free markets don’t work.
In hopes of helping them understand what’s really going on, I try to explain to them that an unfettered market involves consumers and producers directly interacting with their own money in an open and competitive environment.
I then explain why that’s not a description of the U.S. system. Not even close. As I noted in Part I, consumers directly finance only 10.5 percent of their healthcare expenses. Everything else involves a third-party payer thanks to government interventions such as Medicare, Medicaid, the healthcare exclusion, the Veterans Administration, etc.
Obamacare then added another layer of intervention to the existing mess. By my rough calculations, that costly boondoggle took the country from having a system that was 68-percent controlled and dictated by government to a system where government dictates and controls 79 percent of the system.
This is very relevant because Republicans in Washington are now trying to “repeal and replace” Obamacare, but they’re confronting a very unpleasant reality. Undoing that legislation won’t create a stable, market-driven healthcare system. Instead, we’d only be back to where we were in 2010 – a system where government would still be the dominant player and market forces would be almost totally emasculated.
The only difference is that Republicans would then get blamed for everything that goes wrong in the world of healthcare rather than Obama and the Democrats (and you better believe that’s a big part of the decision-making process on Capitol Hill).
Yes, the GOP plan would save some money, which is laudable, but presumably the main goal is to have a sensible and sustainable healthcare system. And that’s not going to happen unless there’s some effort to somehow unravel the overall mess that’s been created by all the misguided government policies that have accumulated over many decades.
This isn’t a new or brilliant observation. Milton Friedman wrote about how government-controlled healthcare leads to higher costs and lower quality back in 1977, but I can’t find an online version of that article, so let’s look at what he said in a 1978 speech to the Mayo Institute.
I realize that many people won’t have 45 minutes of spare time to watch the entire video, so I’ll also provide some excerpts from a column Friedman wrote back in the early 1990s that makes the same points. He started by observing that bureaucratic systems have ever-rising costs combined with ever-declining output.
…a study by Max Gammon…comparing input and output in the British socialized hospital system…found that input had increased sharply, while output had actually fallen. He was led to enunciate what he called “the theory of bureaucratic displacement.” In his words, in “a bureaucratic system . . . increase in expenditure will be matched by fall in production. . . . Such systems will act rather like `black holes,’ in the economic universe, simultaneously sucking in resources, and shrinking in terms of `emitted production.'” …concern about the rising cost of medical care, and of proposals to do something about it — most involving a further move toward the complete socialization of medicine — reminded me of the Gammon study and led me to investigate whether his law applied to U.S. health care.
Friedman then noted how this bureaucratic rule operated in the United States after the healthcare exclusion was adopted during World War II.
Even a casual glance at figures on input and output in U.S. hospitals indicates that Gammon’s law has been in full operation for U.S. hospitals since the end of World War II… Before 1940, input and output both rose, input somewhat more than output, presumably because of the introduction of more sophisticated and expensive treatment. The cost of hospital care per resident of the U.S., adjusted for inflation, rose from 1929 to 1940 at the rate of 5% per year; the number of occupied beds, at 2.4% a year. Cost per patient day, adjusted for inflation, rose only modestly. The situation was very different after the war. From 1946 to 1989, the number of beds per 1,000 population fell by more than one-half; the occupancy rate, by one-eighth. In sharp contrast, input skyrocketed. Hospital personnel per occupied bed multiplied nearly seven-fold and cost per patient day, adjusted for inflation, an astounding 26-fold.
Friedman then explained that the adoption of Medicare and Medicaid hastened the erosion of market forces.
One major engine of these changes was the enactment of Medicare and Medicaid in 1965. A mild rise in input was turned into a meteoric rise; a mild fall in output, into a rapid decline. …The federal government’s assumption of responsibility for hospital and medical care for the elderly and the poor provided a fresh pool of money, and there was no shortage of takers. Personnel per occupied bed, which had already doubled from 1946 to 1965, more than tripled from that level after 1965. Cost per patient day, which had already more than tripled from 1946 to 1965, multiplied a further eight-fold after 1965. Growing costs, in turn, led to more regulation of hospitals, further increasing administrative expense.
Remember, Friedman wrote this article back in 1991. And the underlying problems have gotten worse since that time.
So what’s the bottom line? Friedman pointed out that the problem is too much government.
The U.S. medical system has become in large part a socialist enterprise. Why should we be any better at socialism than the Soviets?
And he explained that there’s only one genuine solution.
The inefficiency, high cost and inequitable character of our medical system can be fundamentally remedied in only one way: by moving in the other direction, toward re-privatizing medical care.
Some readers may be skeptical. Even though he cited lots of historical evidence, perhaps you’re thinking Friedman’s position is impractical.
So let’s fast forward to 2017 and look at some very concrete data assembled by Mark Perry of the American Enterprise Institute. He looks at medical costs over the past 18 years and compares what’s happened with prices for things that are covered by third-party payer (either government or government-distorted private insurance) and prices for cosmetic procedures that are financed directly by consumers.
As you can see, the relative price of health care generally declines when people are spending their own money and operating in a genuine free market. But when there’s third-party payer, relative prices rise.
Perry explains the issue very succinctly.
Cosmetic procedures, unlike most medical services, are not usually covered by insurance. Patients paying 100% out-of-pocket for elective cosmetic procedures are cost-conscious, and have strong incentives to shop around and compare prices at the dozens of competing providers in any large city. Providers operate in a very competitive market with transparent pricing and therefore have incentives to provide cosmetic procedures at competitive prices. Those providers are also less burdened and encumbered by the bureaucratic paperwork that is typically involved with the provision of most standard medical care with third-party payments. Because of the price transparency and market competition that characterizes the market for cosmetic procedures, the prices of most cosmetic procedures have fallen in real terms since 1998, and some non-surgical procedures have even fallen in nominal dollars before adjusting for price changes. In all cases, cosmetic procedures have increased in price by far less than the 100.5% increase in the price of medical care services between 1998 and 2016 and the 176.6% increase in hospital services.
In other words, a free market can work in healthcare. And it gives us falling prices and transparency rather than bureaucracy and inefficiency. Maybe when they’ve exhausted all other options, Republicans will decide to give freedom a try.
P.S. If you want to get a flavor for how competition and markets generate better results, watch this Reason TV video and read these stories from Maine and North Carolina.
And as Milton Friedman wisely observed, that approach (known as “third-party payer”) undermines normal market incentives for lower costs. Indeed, it’s a green light for ever-higher costs, which is exactly what we see in the parts of the healthcare system where government programs or insurance companies pick up most of the tab.
For what it’s worth, I’m not overflowing with confidence that the new Obamacare-replacement proposal from Republicans will have much impact on the third-party payer crisis. And it probably doesn’t solve some of the Obamacare-specific warts in the system. If you want to get depressed about those issues, read what Michael Cannon, Philip Klein, and Christopher Jacobs have written about the new GOP plan.
But healthcare in America is also a fiscal issue. And if we’re just looking at the impact of the American Health Care Act on the burden of government spending and taxes, I’m a bit more cheerful.
The Congressional Budget Office released its official score on the impact of the legislation. Here’s the excerpt that warmed my heart.
Outlays would be reduced by $1.2 trillion over the period, and revenues would be reduced by $0.9 trillion. The largest savings would come from reductions in outlays for Medicaid and from the elimination of the Affordable Care Act’s (ACA’s) subsidies for nongroup health insurance. … parts of the legislation would repeal or delay many of the changes the ACA made to the Internal Revenue Code… Those with the largest budgetary effects include: • Repealing the surtax on certain high-income taxpayers’ net investment income; • Repealing the increase in the Hospital Insurance payroll tax rate for certain high-income taxpayers; • Repealing the annual fee on health insurance providers; and • Delaying when the excise tax imposed on some health insurance plans with high premiums would go into effect.
And fellow wonks will be interested in this table.
By the way, the “two cheers” in the title may be a bit too generous. After all, there should be full reform of Medicare and Medicaid. Though I suppose some of that can happen (at least Medicaid, hopefully) as part of the regular budget process.
It’s also unfortunate that Republicans are creating a new refundable tax credit (and when you see the term “refundable tax credit,” that generally is a sneaky euphemism for more government spending that is laundered through the tax code, sort of like the EITC) to replace some of the Obamacare subsidies that are being repealed.
So it’s far from ideal.
For those who want to see the glass as being half-full rather than half-empty, however, Ryan Ellis has a very upbeat assessment in a column for Forbes.
It’s a net spending cut of over $1.2 trillion and a net tax cut of nearly $900 billion over the next decade. …the score shows that the AHCA would be a large and permanent tax cut for families and employers….This should lower the tax revenue baseline considerably, perhaps even by half a percentage point of the economy.
I like starving the beast, so I agree this is a good thing.
And I also agree with Ryan that the resulting lower tax burden on dividends and capital gains is very positive. After all, double taxation is probably the most pernicious feature of the internal revenue code.
The most pro-growth tax cut in the bill is the elimination of the so-called “NIIT” or “net investment income tax.” It adds on a 3.8 percentage point surtax on savers and investors. By eliminating NIIT, the bill cuts the capital gains and dividends tax from 23.8 percent in 2017 to 20 percent in 2018 and beyond. …The contribution limit to HSAs is doubled, from nearly $7000 for families today to $14,000 starting in 2018.
But I’ll close with some sad news. If the legislation is approved, that probably means no more Obamacare-related humor. If this makes you sad, you can easily spend about 30 minutes enjoying Obamacare cartoons, videos, and jokes by clicking here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, and here.
I call it the “First Theorem of Government,” and I think it accurately reflects the real purpose and operation of government. Except I probably should have added lobbyists and contractors. And it goes without saying (though I probably should have said it anyhow) that politicians are the main beneficiaries of this odious racket.
I think this theorem has stood the test of time. It works just as well when Republicans are in charge as it does when Democrats are in charge.
But it doesn’t describe everything.
For instance, Republicans have won landslide elections in recent years by promising that they will repeal Obamacare the moment they’re in charge. Well, now they control both Congress and the White House and their muscular rhetoric has magically transformed into anemic legislation.
This is very disappointing and perhaps I’ll share some of Michael Cannon’s work in future columns about the policy details, but today I want to focus on why GOP toughness has turned into mush.
In part, this is simply a reflection of the fact the rhetoric of politicians is always bolder than their legislation (I didn’t agree with 98 percent of what was said by Mario Cuomo, the former Governor of New York, but he was correct that “You campaign in poetry. You govern in prose.”)
But that’s just a small part of the problem. The real issue is that it’s relatively easy for GOP politicians to battle against proposed handouts and it’s very difficult to battle against existing handouts. That’s because government goodies are like a drug. Recipients quickly get hooked and they will fight much harder to preserve handouts than they will to get them in the first place.
And that’s the basic insight of the “Second Theorem of Government.”
Here’s a recent interview on FBN. The topic is the Republican reluctance to fully repeal Obamacare. I only got two soundbites, and they both occur in the first half of the discussion, but you can see why I was motivated to put forth the new theorem.
Simply stated, I’m disappointed, but I’m more resigned than agitated because this development was so sadly predictable.
And here are a couple of follow-up observations. I guess we’ll call them corollaries to the theorem.
You break it, you buy it – Government intervention had screwed up the system well before Obamacare was enacted, but people now blame the 2010 law (and the Democrats who voted for it) for everything that goes wrong with healthcare. Republicans fear that all the blame will shift to them if their “Repeal and Replace” legislation is adopted.
Follow the money – What’s partly driving GOP timidity is their desire not to anger many of the interest groups – such as state governments, hospitals, doctors, insurance companies, etc – who benefit from various Obamacare handouts. That’s what is motivating criticism for politicians such as Ohio’s John Kasich and Alaska’s Lisa Murkowski.
Don’t throw the baby out with the bathwater – The “Cadillac Tax” is the one part of Obamacare that’s worth preserving because it will slowly cut back on the distorting tax preferences that lead to over-insurance and third-party payer. For what it’s worth, the GOP plan retains that provision, albeit postponed until 2025.
For these reasons (as well as other corollaries to my theorem), I’m not brimming with optimism that we’ll get real Obamacare repeal this year. Or even substantive Obamacare reform.
P.S. Now you know what I speculated many years ago that Obamacare would be a long-run victory for the left even though Democrats lost many elections because of it. I sometimes hate when I’m right.
And if you want to be even more specific, the fastest-growing entitlement program is Medicaid, which was originally supposed to be a very small program to subsidize health care for poor people but has now metastasized into a budget-gobbling fiscal disaster. Arguably, it’s the entitlement program most in need of reform.
So how big is the problem? Enormous if you look at the numbers from the National Association of State Budget Officers.
States increased their spending in fiscal year 2015 by the biggest margin in more than 20 years, but most of the increase was thanks to huge leaps in Medicaid spending under the first full year of the Affordable Care Act (ACA). Spending increased last fiscal year, which ended on June 30 for most states, by 7.8 percent, according to new estimates from the National Association of State Budget Officers (NASBO). It’s the biggest boost since 1992 and was thanks to a 15.1 percent increase in Medicaid spending, much of that paid for via federal Medicaid funds. Illinois, Michigan, Kentucky, Nevada and Oregon saw more than 30 percent increases in federal funding because they expanded Medicaid under the ACA. But 2015 was also a year where states were putting up more of their own money again.
Here’s the chart showing which outlay categories grew the fastest.
The article points out that spending is outpacing revenue.
On average, state revenues aren’t keeping pace with spending; NASBO estimates General Fund revenues will increase by just 3.8 percent.
Though the real problem is that spending is expanding faster than the private sector, which is the opposite of what is called for by my Golden Rule.
One of the reasons Medicaid grows so fast is that the program is split between Washington and the states, which both picking up a share of the cost. This may sound reasonable, but it creates a very perverse incentive structure since politicians at both levels can vote to expand the spending burden while only having to provide part of the cost.
The National Center for Policy Analysis explains how this system produces bad decisions.
Medicaid has a horrible financing mechanism: Federal transfers to states are not based on the number of poor people, or any other reasonable calculation. Instead, they depend on the amount of its own taxpayers’ money a state spends. Traditionally, when California spent $1 on Medi-Cal, the federal government kicked in $1. …So, state politicians hike taxes and spending on their own citizens in order to get as much funding as possible from people in other states (via the feds). Hospitals and Medicaid MCOs maximize this by agreeing to a state tax on themselves, which the state uses to ratchet up the federal funding. After multiplication, the money goes right back to these providers. …Stopping this wild spending growth requires fundamental reform to Medicaid’s financing. Congressional Republicans have proposed “block grants,” whereby states would get federal Medicaid transfers based on their population of poor residents, not how much they gouge out of their own people.
But unless that kind of reform happens, the program will continue to grow and become an ever-larger fiscal burden.
Heritage Action has more details on the perverse incentives of the current system.
…the federal government promises to reimburse states for a majority of their Medicaid spending, most of which involves reimbursements to health care providers. Therefore, states collude with health care providers in the following manner: they tell providers that they will tax them (so-called “provider taxes”), bringing in more revenue to the state. The state then promises to filter that money back to those same providers in the form of higher Medicaid reimbursements. States then bill the federal government for this added cost. Because the federal government provides more than 50% of total Medicaid funding, both state governments and Medicaid providers are made better off by the arrangement, while the federal government is stuck footing a larger bill it had no part in creating.
Though I partially disagree with the assertion that the feds are blameless. After all, it was politicians in Washington who created this wretched system, including the reimbursement rules that states manipulate.
The net result of all this is a nightmare for federal taxpayers, but states also are losing out when you consider the long-run consequences. And that’s even true with the Medicaid expansions contained in Obamacare, which supposedly were going to be financed almost entirely by Uncle Sam. The Wall Street Journalreports.
…the Affordable Care Act was designed to essentially bribe states to expand their Medicaid programs: The feds offered to pay 100% of additional costs through 2016, dropping to 90% by 2020. This “free money” prompted 30 states and the District of Columbia to take the deal. Democratic activists have joined with state hospital lobbies to pressure lawmakers in the remaining 20 state capitals to follow.
But free money can be very expensive.
Consider the experience of the states that did expand Medicaid. “At least 14 states have seen new enrollments exceed their original projections, causing at least seven to increase their cost estimates for 2017,” the Associated Press reported in July. The AP says that California expected 800,000 new enrollees after the state’s 2013 Medicaid expansion, but wound up with 2.3 million. Enrollment outstripped estimates in New Mexico by 44%, Oregon by 73%, and Washington state by more than 100%. This has blown holes in state budgets. Illinois once projected that its Medicaid expansion would cost the state $573 million for 2017 through 2020. Yet 200,000 more people have enrolled than were expected, and the state has increased its estimated cost for covering each. The new price tag? About $2 billion… Enrollment overruns in Kentucky forced officials to more than double the anticipated cost of the state’s Medicaid expansion for 2017, the AP reports, to $74 million from $33 million. That figure could rise to $363 million a year by 2021. In Rhode Island, where one-quarter of the state’s population is now on Medicaid, the program consumes roughly 30% of all state spending, the Providence Journal reports. To plug this growing hole, Rhode Island has levied a 3.5% tax on insurance policies sold through the state’s ObamaCare exchange.
Interestingly, Obamacare is causing pro-big government states to dig even deeper fiscal holes.
The National Center for Policy Analysis has some remarkable data on this development.
States that expanded Medicaid tend to have per capita state spending that’s about 17 percent higher than non-expansion states. …In 2004, expansion states had median per capita tax collections (both state and local) of 19 percent more than non-expansion states. By 2012, this gap had widened with expansion states collecting 28 percent more taxes per capita than non-expansion states. Moreover, since 2008 expansion states have moved to increase taxes, while non-expansion states have reduced taxes slightly.
Unsurprisingly, the states that are making government bigger are experiencing slower growth.
In 2001 expansion states had real median income that was nearly 13 percent higher than non-expansion states. However, by 2013 this gap had narrowed to just over 9 percent. Expansion states have historically had slightly lower poverty rates, but the difference was only 1 percentage point by 2012 (12.9 percent vs. 13.9 percent). Non-expansion states, although slightly poorer, have lower unemployment than expansion states (6.7 percent versus 7.2 percent).
Another point worth mentioning is that the program isn’t even a good deal for the poor according to Scott Atlas at the Hoover Institution. Here’s some of what he wrote for the Wall Street Journal.
Americans should be more worried than ever about Medicaid… The cost of the $500 billion program is expected to rise to $890 billion by 2024… Yet more spending doesn’t necessarily mean better care for beneficiaries… The expansion of Medicaid is one of the most misguided parts of ObamaCare… Some 55% of doctors in major metropolitan areas refuse to take new Medicaid patients… Medicaid enrollees who manage to see a doctor typically experience outcomes worse than those under private insurance. That means more in-hospital deaths, more complications from surgery, worse posttreatment survival rates, and longer hospital stays than similar patients with private insurance. A randomized study by the Oregon Health Study Group showed that having Medicaid did not significantly improve patients’ physical health compared with those without insurance.
The proverbial icing on this foul-tasting cake is the way the program enables staggering amounts of fraud and theft.
I’ve written about this before (including how foreigners are bilking the system). But here are some fresh details from the Wall Street Journal.
…one of our favorite political euphemisms is “improper payments.” That’s how Washington airbrushes away the taxpayer money that flows each year to someone who is not eligible, or to the right beneficiary in the wrong amount, or that disappears to fraud or federal accounting ineptitude. Now thanks to ObamaCare, improper payments are soaring. Last week the Health and Human Services Department published an “alert” warning that the improper payment rate for Medicaid in 2016 will likely hit 11.5%. That’s nearly double the 5.8% rate as recently as 2013… The 11.5% for 2016 is likely an underestimate given that HHS’s goal last year was 6.7% and instead scored 9.8%, which amounts to $29.1 billion. The dollar amount of improper payments in Medicaid was bound to rise because ObamaCare vastly opened eligibility. In 2015 enrollment climbed by 13.8% and one of five Americans are now covered by the program. …In recent audits of Medicaid in Arizona, Florida, Michigan and New Jersey, the GAO uncovered 50 dead people who recouped at least $9.6 million in benefits after they died; 47 providers who registered foreign addresses as their location of service in places such as Saudi Arabia; and $448 million bestowed on 199,000 beneficiaries with fake Social Security numbers—12,500 of which had never been issued by the Social Security Administration.
But as bad as all this sounds, it can get worse.
If HHS tries hard enough, maybe the department can match the failure rate for school lunches (15.7%) or the Earned Income Tax Credit (23.8%).
And Kevin Williamson of National Reviewadds some acidic observations.
…the criminal — and I do not use the word figuratively — administration of Medicaid by the Obama administration. …improper payments under Medicaid have become so common that they will account this year for almost 12 percent of total Medicaid spending — just shy of $140 billion. …That rate has doubled in only a few years…12 percent in improper payments isn’t an error rate — it’s a malfeasance rate. …If improper and illegal federal payments were an economy of their own, that economy would be bigger than Hungary’s… The Obama administration is not lifting a pinky to do anything about this, even though analysts such as John Hood have — for years — been arguing that it is necessary and possible to reform this mess. As the Wall Street Journal has reported, we don’t even verify that doctors billing Medicaid for services rendered are actually doctors. In many cases, we do not do much to verify that their patients actually, you know, exist. We’ve paid untold billions of dollars to “clinics” that turn out to be little more — or nothing more — than post-office boxes and prepaid cell phones. And as bad as that 12 percent rate is, some policy scholars believe that it is in fact probably worse.
Kevin observes that this system is good for the Poverty Pimps.
…the real problem with the welfare state is not the poor people receiving checks — it’s everybody in the middle, the vast array of government employees, their union allies, contractors, and third parties who earn six-, seven-, eight-, or nine-figure paydays taking their cuts of money we think we’re spending on the poor. This is an enormous criminal conspiracy against the American people and the public fisc.
You might think that fixing this fraud would be an area for bipartisan cooperation.
But the sad reality is that fraud is a feature, not a bug. Politicians like the fact that scam artists in their states and district are stealing healthcare money from taxpayers. After all, recipients of the loot can be registered voters and campaign contributors.
So what’s the best way of fixing this mess?
Will big tax hikes solve the problems? If the problem is that America isn’t enough like France, then the answer is yes.
But if the problem is that government already is too much of a burden and that it would be a good idea to at least slow down the rate at which America becomes France, then the answer is genuine entitlement reform.
P.S. For all intents and purposes, block granting Medicaid is a partial repeal of Obamacare. Just in case you wanted an additional reason to support reform.
Based on what’s been happening, those of us who have been warning about the fiscal burden of Medicaid, Medicare, and Obamacare could rest on our laurels and say “we told you so.” But it’s a Pyrrhic victory because being right means bad news for the country.
Earlier this year, The Hillreported some very sobering news about the ever-growing burden of health entitlements.
Spending on federal healthcare programs outpaced spending on Social Security for the first time in 2015, according to an expansive report from the congressional budget scorekeeper released Monday. The government spent $936 billion last year on health programs including Medicare, Medicaid and subsidies related to the Affordable Care Act, a jump of 13 percent from 2014, according to the Congressional Budget Office. Spending on Social Security, in contrast, totaled $882 billion, the Congressional Budget Office (CBO) reported.
Let’s look at just one example of why the fiscal burden of health entitlements keeps growing so rapidly.
According to new data, the portion of Obamacare that expanded Medicaid is generating a torrent of new spending.
Charles Blahous is a former Trustee for Social Security and Medicare Given his inside-the-belly-of-the-beast familiarity with entitlement programs, what he’s written should be especially alarming.
The implementation of major legislation such as the Affordable Care Act (ACA) often results in fiscal outcomes that differ significantly from prior projections. …Recall that the ACA considerably expanded Medicaid eligibility… It turns out that the 2015 per-capita cost of this Medicaid expansion is a whopping 49% higher than projections made just one year before. This disclosure can be found on page 27 of the 2015 Actuarial Report for Medicaid, released this July.
Here’s the chart showing how much higher per-recipient spending will be according to the new numbers.
Blahous goes through a lot of technical information to explain why the previous forecasts were so inaccurate.
But here’s the part that I think is most important to understand. Obamacare created a free lunch for states, at least in the short run. So we shouldn’t be surprised that many states have been seduced into participating and that they’re now spending money like drunken sailors.
Basically states established far higher expenditure requirements for the expansion population than the federal government expected, by positing that beneficiaries would be in need of more health services. Why did this happen? Remember, the ACA established an initial 100% federal matching payment for state Medicaid expansion costs, contrasting with historical federal match rates that averaged 57%. Even when the feds paid 57% of the bill there was a longstanding concern that states were insufficiently accountable for their cost-expanding decisions, with much of that cost being shifted to federal taxpayers. But the ACA’s current 100% match means that states make the decisions about expanding Medicaid while the federal government picks up all the costs. Even after the ACA is fully phased in, the feds will still pay for 90%. Under such arrangements, cost overruns are predictable.
So what’s the obvious conclusion?
Having federal taxpayers pick up between 90-100% of the cost of state Medicaid expansions was one of many questionable policy decisions made in the ACA. It’s also proving to be much more expensive than the federal government expected.
Brian Blase of the Mercatus Center also has a grim assessment on the numbers.
The Department of Health and Human Services’ (HHS) annual report on Medicaid’s finances contains a stunning update: the average cost of the Affordable Care Act’s Medicaid expansion enrollees was nearly 50% higher in fiscal year (FY) 2015 than HHS had projected just one year prior. Specifically, HHS found that the ACA’s Medicaid expansion enrollees cost an average of $6,366 in FY 2015—49% higher than the $4,281 amount that the agency projected in last year’s report. The government’s chief financial experts appear not to have anticipated how states would respond to the federal government’s 100% financing of the cost of people made eligible for Medicaid by the ACA. It appears that the enhanced federal funding for the ACA expansion population has led states to set outrageously high capitation rates—the amount government pays insurers—for the ACA Medicaid expansion population.
Blase points out that this goes beyond the traditional failure of bureaucrats to accurately anticipate behavioral changes when politicians give away other people’s money.
There’s also some sleazy maneuvers to funnel money to special interest groups.
…the amounts…suggest that states are inappropriately funneling federal taxpayer money to insurers, hospitals, and other health care interests through the ACA Medicaid expansion. …The health care interest groups within the states, particularly hospitals and insurers, benefit from the higher rates while federal taxpayers are left footing the bill. …Moreover, the elevated federal reimbursement rate removes the incentives for states to make sure that insurers are not overspending on providers since overpayments come at the expense of federal, not state, taxpayers.
And most of the new spending does wind up in the pockets of the interest groups.
Recent evidence that new Medicaid enrollees only receive about 20 to 40 cents of benefit for each dollar of spending on their behalf.
But even the small fraction that goes to consumers doesn’t seem to have much positive impact on their health according to one major new study.
Medicaid expansion in Oregon was not related to significant health improvements.
So what does all this mean?
Obamacare has been a disaster. This column has been a look at how just one provision has backfired on taxpayers.
And just as bureaucrats are grossly incompetent at estimating the revenue impact of changes in tax law, they’re also grossly incompetent at predicting behavioral changes when expanding entitlement programs.
Some of us, for what it’s worth, warned about this as Obamacare was being debated.
P.S. Since I don’t want to be a naive rube, allow me to acknowledge there’s an alternative explanation for consistently inaccurate fiscal forecasts from the government.
But for ordinary people, what probably matters most is household income. And if you look at the median household income numbers for the United States, Obamanomics is a failure. According to the Census Bureau’s latest numbers, the average family today has less income (after adjusting for inflation) than when Obama took office.
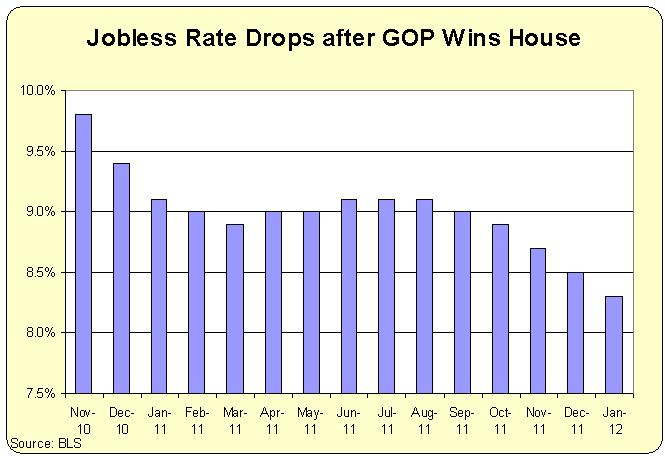
In an amazing feat of chutzpah, however, the President is actually arguing that he’s done a good job with the economy. His main talking point is that the unemployment rate is down to 4.7 percent.
Yet as discussed in this Blaze TV interview, sometimes the unemployment rate falls for less-than-ideal reasons.
But he can be blamed for the fact that the numbers haven’t recovered, as would normally happen as an economy pulls out of a recession. This is a rather damning indictment of Obamanomics.
By the way, I can’t resist commenting on what Obama said in the soundbite that preceded my interview. He asserted that “we cut unemployment in half years before a lot of economists thought we could.”
In effect, the President airbrushed history and then tried to take credit for something that happened, at least in part, because of policies he opposed.
Wow.
One final point. I was asked in the interview which policy deserves the lion’s share of the blame for the economy’s tepid performance and weak job numbers.
I wasn’t expecting that question, so I fumbled around a bit before choosing Obamacare.
It’s even been bad for some of the special interest groups that backed the legislation. The big insurance companies supported the law, for instance, because they thought it would be good to have the government force people to buy their products.
And these corrupt firms even got a provision in the law promising bailouts from taxpayers if the Obamacare system didn’t work.
But the companies mistakenly assumed their sleazy pact with Obama, Pelosi, and Reid was permanent. Fortunately, their Faustian bargain appears to be backfiring.
Senator Marco Rubio has led the fight to stop bailouts for the big insurance companies.
Here are some excerpts from his recent column in the Wall Street Journal.
Six years after being signed into law, ObamaCare is a costly and unsustainable disaster. …ObamaCare is also bringing out corporate America’s worst crony-capitalist impulses. The health-insurance lobby has teamed up with trial lawyers to sue the federal government—through individual lawsuits and a $5 billion class action—for not following through on a sweetheart bailout deal buried in the law. This provision of ObamaCare would have required taxpayers to bail out insurers.
But in a rare victory for taxpayers, the Florida Senator got the law changed to restrict bailouts.
My conservative colleagues and I sounded the alarm about the likelihood of a taxpayer-funded bailout of health insurers (and were mocked as Chicken Littles for it). …When it came time to pass a spending bill at the end of 2014, we succeeded in making it the law of the land that the ObamaCare bailout program could not cost taxpayers a single cent—which ended up saving taxpayers $2.5 billion. In December of last year, we came back and repeated the feat. Now I am urging leaders in both the House and Senate to make this a priority and stop the bailout a third time.
As you might imagine, there’s a counterattack by the corrupt insurance companies that conspired with the White House to impose Obamacare on the nation.
…the health-insurance companies are suing to try to get their bailout…professional attorneys from the Congressional Research Service…said that the administration’s practice of making other payments to insurers under the ObamaCare reinsurance program “would appear to be in conflict with the plain text” of the law. …Health insurers can hire all the high-paid trial lawyers they want, but they will run into a constitutional buzz saw: America’s founding document grants Congress the power of the purse… Health-insurance companies need to wake up to the reality that this…money they are fighting for, and that the Obama administration is trying to weasel a way to somehow give them, belongs to taxpayers. Taxpayers get to decide—through me and others in Congress—whether to bail them out. And the people have spoken: No, we will not bail out health insurance companies for ObamaCare’s failures.
Amen to Senator Rubio.
Let’s hope Congress continues to oppose bailouts, and let’s also hope the White House isn’t successful in somehow giving our money to the big insurance companies.
Speaking of which, here’s what Investor’s Business Dailywrote about the bailout controversy.
Right when you think Washington can’t get any worse, it does. That much was evident at a recent U.S. House of Representatives committee hearing into the Obama administration’s bailout of private health insurance companies. It’s a textbook case of government officials ignoring federal law to put special interests before the interests of American taxpayers and families.
Here’s how the mess was created…and how the Obama White House chose to respond.
Thanks to the Affordable Care Act’s labyrinthine mandates, health insurance companies have collectively lost billions of dollars on the exchanges, leading to an increasing number of them limiting their participation in or exiting the exchanges altogether. As a result, many insurers have demanded larger subsidy payments. …responding to insurance industry demands — in November the Obama administration promised to “explore other sources of funding” for payments to insurers. Yet rather than work with Congress, the administration flouted the law entirely — and in this case, that means using tax dollars to bail out insurers left on the exchanges. CMS simply decided to ignore the law.
Unfortunately, ordinary people don’t have that option.
They simply pay more to get less.
Meanwhile, Americans rightly wonder who’s looking out for them. Premiums have actually risen faster in the five years after passage of the Affordable Care Act than in the five years before, while deductibles average nearly $3,000 for the most popular exchange plans.
Speaking of special deals, let’s look at another Obamacare rescue for a privileged group.
Bob Moffit of the Heritage Foundation explains the contortions needed to keep health insurance subsidies flowing to Capitol Hill.
…one scandal is truly bipartisan: How key administration and congressional officials connived to create, under cover of the Affordable Care Act, also known as Obamacare, special health insurance subsidies for members of Congress.
Here’s the background.
Rushing to enact the giant Obamacare bill in March 2010, Congress voted itself out of its own employer-sponsored health insurance coverage—the Federal Employees Health Benefits Program. …But in pulling out of the Federal Employees Health Benefits Program, they also cut themselves off from their employer-based insurance contributions.
Subjecting themselves and their staff to Obamacare may have been smart politics, if only to avoid the charge of hypocrisy, but that created a different problem.
Obamacare’s insurance subsidies for ordinary Americans are generous, but capped by income. No one with an annual income over $47,080 gets a subsidy. That’s well below typical Capitol Hill salaries. Members of Congress make $174,000 annually, and many on their staff have impressive, upper-middle-class paychecks. …Realizing what they had done, congressional leaders sought desperately to get fatter taxpayer subsidies in the Obamacare exchange system. …The standard excuse was that, without a special “sweetener,” a Capitol Hill “brain drain” would ensue; the best and brightest would flee to the private sector to get more affordable employment-based coverage.
Gee, it would have been a shame if the people who have screwed up public policy had to get jobs in the private sector (or, more likely, the parasitic lobbying sector).
But the law oftentimes is not an obstacle when the Obama White House wants something to happen.
…at a July 31 closed-door meeting with Senate Democrats, President Barack Obama had promised he would “fix” the mess they made of their health coverage. So, on Aug. 7, 2013, just as Congress was getting out of town for the August recess, the Office of Personnel Management ruled that members of Congress and staff enrolled in the exchange program would get Federal Employees Health Benefits Program subsidies, even though they were no longer in the program.
But how exactly did the White House evade the law?
…the Office of Personnel Management declared that Congress and staff were eligible to enroll in the Washington, D.C., “SHOP” Exchange, a health insurance exchange reserved for small businesses with fewer than 50 employees. The exchange offers special insurance subsidies to participating small businesses. The problem was, of course, that Congress is not a “small business,” at least under any clinically sane definition of the term, and no section of the Affordable Care Act provided for any congressional exemption from the ban on large employer participation in the SHOP exchanges.
By the way, as a former staffer on Capitol Hill, I do have some sympathy for the lower-level folks who didn’t create the Obamacare mess and would suddenly be in a position of having to pay all their health costs out of pocket if the law was obeyed.
But that’s not a reason to engage in legal chicanery.
And it seems we get more bad news every day, as noted in a new editorial from Investor’s Business Daily.
ObamaCare rates will skyrocket next year, according to its former chief. Enrollment is tumbling this year. And a big insurer is quitting most exchanges. That’s what we learned in just the past few days.
Why do we know these three bad things are happening? Because that’s what we’re being told by Mary Tavenner, the former head of the Center for Medicare and Medicaid Services for the Obama Administration who has now cashed out and is pimping for the health insurance companies that got in bed with the White House to foist Obamacare on the American people.
IBD gives us the sordid details.
Why will 2017 rates spike even higher? In addition to the cost of complying with ObamaCare’s insurance regulations and mandates, there’s the fact that the ObamaCare exchanges have failed to attract enough young and healthy people needed to keep premiums down. Plus, two industry bailout programs expire this year, Tavenner notes. Oh, and she admits that people are gaming ObamaCare just like critics said they would: buying coverage after they get sick — since insurance companies can no longer turn them down or charge them more — then dropping it when they’re done with treatments. “That churn increases premiums. So you have to kind of price over that.”
And that’s just one slice of bad news.
Here’s more.
ObamaCare enrollment has already dropped an average of more than 14% in five states since February — a faster rate of decline than last year — as people get kicked off for not paying premiums. Finally, we learned on Tuesday that UnitedHealth Group (UNH) is planning to drop out of almost every ObamaCare market it currently serves after losing $1 billion on those policies. …Skyrocketing premiums, fewer choices in the marketplace, and people fleeing ObamaCare in droves after signing up. This isn’t exactly what Obama promised when he signed ObamaCare into law.
For those who were paying attention, none of this is a surprise. It was always a fantasy to think that more government intervention was going to improve a healthcare system that already was cumbersome and expensive because of previous government interventions.
By the way, IBD isn’t the only outlet to notice the ongoing disaster of Obamacare.
Let’s look at some other recent revelations.
Chris Jacobs writes that “For millions of Americans, the Left’s insurance utopia has rapidly deteriorated into a bleak dystopia” and that “the ‘cheaper prices’ that the president promised evaporated as quickly as the morning dew.”
John Graham explains that “CBO estimates Obamacare will leave 27 million uninsured through 2019 – an increase of almost one quarter” and that “CBO estimates 68 million will be dependent on the program this year through 2019 – an increase of almost one third in the welfare caseload.”
Betsy McCaughey opines that, “Obamacare is already hugely in the red. …over the next ten years Obamacare will add $1.4 trillion to the nation’s debt” and that “Insurers struggling with Obamacare are already drastically reducing your choice of doctors and hospitals to cut costs.”
Devon Herrick reveals that “Obamacare has caused more people to reach for their wallets after a medical encounter — not less” and that “all but the most heavily subsidized Obamacare enrollees would be better off financially if they skipped coverage and pay for their own medical care out of pocket.”
Jeffrey Anderson observes that “it seems possible that Obamacare has actually reduced the number of people with private health insurance” and that “Obamacare is basically an expensive Medicaid expansion coupled with 2,400 pages of liberty-sapping mandates.”
John Goodman notes that “Prior to Obamacare, many employers of low-wage workers offered their employees a “mini med” plan, covering, say, the first $25,000 of expenses” and that “Those plans are now gone… employees…are…completely uninsured”
The CEO of CKE Restaurants warns that “fewer people buying insurance through the exchanges, the economics aren’t holding up” and that “Ten of the 23 innovative health-insurance plans known as co-ops—established with $2.4 billion in ObamaCare loans—will be out of business by the end of 2015 because of weak balance sheets.”
Critics of Obamacare now get to say “we told you so.”
…conservatives screamed a simple fact from the rooftops: Obamacare will not work. No one wanted to listen then, but their warnings are now coming into fruition. Obamacare, as constructed, attempted to fix a dysfunctional health care payment system by creating an even more complicated system on top of it, filled with subsidies, coverage mandates, and other artificial government incentives. But its result has been a system that plucked Americans out of coverage they like and forced them to pay more for less. …Taxpayers and insurance customers alike should demand replacing Obamacare with a system that reduces costs and improves quality by injecting actual choice and competition into the insurance market.
I especially like the last part of the excerpt. Which is why we need to go well beyond simply repealing Obamacare if we want to restore market forces to the healthcare sector.
P.S. I wrote about that it’s tragic that so many people are suffering because of Obamacare. I should add that there are some victims who actually are getting what they deserve.
P.P.S. In the long run, I fear taxpayers will be the biggest (and most undeserving) victims.
But those were just the slap-you-in-the-face impossible-to-overlook problems.
As Nancy Pelosi infamously noted, the law needed to pass so we could know what was in it.
And the more we learn about the contents, the more evidence we find that (as shown in this poster) that more government is never the answer.
A new empirical study by scholars at Harvard and Stanford finds that “free” goodies from the government actually have a hefty price tag.
The dependent care mandate…one of the most popular provisions of the 2010 Affordable Care Act…requires that employer-based insurance plans cover health care expenditures for workers with children 26 years old or younger. …there has been little scholarly work measuring the costs and incidence of this mandate and who pays the costs of it. In our empirical work, ….we find that workers at firms with employer-based coverage – whether or not they have dependent children – experience an annual reduction in wages of approximately $1,200. Our results imply that the marginal costs of mandated employer-based coverage expansions are not entirely borne only by the people whose coverage is expanded by the mandate.
Wow, this is worse than I thought. I assumed the pejoratively nicknamed “slacker mandate” wasn’t a big issue because the types of kids getting coverage (ages 19-26) presumably had very low health expenses.
But if average wages at affected firms are $1200 lower than they otherwise would be, that’s a big hit. Maybe Pajama Boys have physical health problems in addition to their mental health problems.
Now let’s look at another higher-than-expected cost, except this time the victims are taxpayers and other health care consumers rather than workers.
Politico has a depressing story of how people have figured out how to game the system
Obamacare customers are gaming the system, buying coverage only after they find out they’re ill and need expensive care… No one knows precisely how many might be manipulating the system, but the plans say they run up much higher medical bills and then jump ship, contributing to double-digit rate increases and financial losses. Health plans also complain some customers are exploiting a three-month “grace period” — when they can keep getting subsidized coverage even if they’ve stopped paying their share of premiums.
In other words, Obamacare is so poorly designed – thanks to subsidies, mandates, and other forms of intervention – that many people can basically wait until they’re sick before signing up.
Then they incur expenses that are covered by taxpayers and/or passed on to other healthcare consumers.
There’s also another group of victims, though I confess that part of me thinks that the insurance companies deserve to suffer since they (like Big Pharma) endorsed Obamacare.
…those trends make the risk pools skew toward sicker, costlier customers — and under Obamacare, plans can no longer deny coverage to those with expensive medical conditions. That problem has been exacerbated by the large numbers of healthier people who are choosing to stay uninsured rather than shell out money for coverage.
Yup, I experience a warm glow of schadenfreude after reading that passage. But I also know that it won’t be good for the American economy and the American people if the market for private health insurance entered an Obamacare-driven death spiral.
Regarding bad news, there’s unfortunately a lot of competition. But if I’m forced to pick the very worst developments, here’s my list.
Resuscitation of the Export-Import Bank – I did a premature victory dance last year when I celebrated the expiration of the Export-Import Bank’s authority. I should have known that corrupt cronyism was hard to extinguish. Sure enough, Republicans and Democrats conspired to re-authorize the Ex-Im Bank and transfer wealth from ordinary Americans to politically connected corporations.
Expansion of IMF authority – I also did a premature victory dance in 2014 when I lauded the fact that Congress did not approve increased bailout authority for the International Monetary Fund. Sadly, as part of the year-end spending agreement, Congress agreed to expand the IMF’s authority so it could continue to push for higher taxes around the world.
Busting the spending caps (again) – When I wrote last August that maintaining the spending caps was a key test of GOP integrity, I should have known that they would get a failing grade. Sure enough, Republicans deliberately fumbled the ball at the goal line and agreed to higher spending. Again.
Supreme Court ignores law to bail out Obamacare (again) – Back in 2012, the Supreme Court had a chance to rule whether Obamacare was an impermissible expansion of the power of the federal government. In a truly odious decision, Chief Justice John Roberts ignored the Constitution’s limits on federal powers and decided we could be coerced to buy health insurance. Last year, he did it again, this time by bailing out a key part of Obamacare by deciding to arbitrarily ignore the wording of the law.
Business-as-usual transportation bill – The desire of Congress to fund pork-barrel transportation projects is at least somewhat constrained by the amount of revenue generated by the gas tax. There was an opportunity for reform in 2015 because proposed spending was much higher than the trajectory of gas tax revenue, but rather than even engage in a discussion of good policy options, politicians merely bickered over what combination of tax hikes and budget gimmicks they could put together to keep the pork projects flowing.
Creeping support on the right for the value-added tax – When I wrote early last year that the 2016 election might create an opportunity for tax reform, I was being hopeful that we might get something close to a simple and fair flat tax. Yet probably the biggest news so far in this election cycle is that a couple of candidates who presumably favor small government – Rand Paul and Ted Cruz – have proposed to impose a value-added tax without fully repealing the income tax.
There’s very little good news to celebrate. Here’s my tragically sparse list, and you’ll notice that my list of victories is heavy on style and light on substance. But let’s take what we can get.
Semi-decent Republican budgets – The budget resolution produced by Congress technically doesn’t embrace specific policies, but the it’s nonetheless noteworthy that the House and Senate approved numbers that – at least conceptually – are based on genuine Medicaid and Medicare reform.
Good election results from the Wolverine State – It was great to see Michigan voters reject a gas tax increase that was supported by the political elite.
A glimmer of reality at the New York Times – I realize I’m scraping the bottom of the barrel in my search for good news, but the fact that the New York Times published a column acknowledging that feminist economic policies backfire against women hopefully is a sign that sensible thinking is possible in the establishment media.
Gun control flopping – It’s great to see that the left has totally failed in its effort to undermine 2nd Amendment rights.
I would offer predictions for 2016, but since my big prediction from last year that we would have gridlock was sadly inaccurate, I think I’ll avoid making a fool of myself this year.
Instead, I feel obliged to issue somewhat of a retraction for my assertion that Obama care is a job killer.
Some of you may be scratching your heads, particularly if you read these passages from an article earlier this week in The Hill.
ObamaCare will force a reduction in American work hours — the equivalent of 2 million jobs over the next decade, Congress’s nonpartisan scorekeeper said Monday. The total workforce will shrink by just under 1 percent as a result of changes in worker participation because of the new coverage expansions, mandates and changes in tax rates, according to a 22-page report released by the Congressional Budget Office (CBO). …the law changes incentives over the years for the workers themselves both in part-time and full-time positions.
So why, then, am I issuing a mea culpa on Obamacare and jobs?
Well, some readers may have concluded from my writings that Obamacare is an absolute job killer.
Yet, as we see from this story in the Kansas City Star, there may be some jobs being created because of the so-called Affordable Care Act. Here are some relevant excerpts.
H&R Block expects more customers to feel the impact of the Affordable Care Act when they do their taxes early next year, providing a source of growth for the Kansas City-based business. A year ago, Block invested in marketing and training its tax preparers… “We think we’re going to start to reap the benefits of that investment,” Block chief executive Bill Cobb said Tuesday during a strategy session with analysts. …the company said an early effort will be aimed at getting back customers the company lost last year.
To be sure, H&R Block isn’t explicitly saying that it will have additional employees, but I think we can infer that some new positions will be created as the company takes advantage of the fact that many taxpayers will be overwhelmed by the complexities and penalties that are part of Obamacare.
With this in mind, I’m going to be very careful in the future to state that the President’s law is a net job killer or a relative job killer.
After all, I wouldn’t want anyone to accuse me of being unfairly or inaccurately critical of government-run healthcare. Even in cases when the jobs being created are evidence of bad legislation rather than a good economic climate.
P.S. I’m not a big fan of H&R Block. Assuming they didn’t support Obamacare, I don’t blame them for enjoying the extra profits they’ll earn because of the law. But the company has supported government rules to block competition in the tax-compliance industry. And I remember many years ago being part of a debate in Louisiana where a representative from H&R Block argued against the flat tax. Gee, I wonder why?
And to bolster the case for reform, we’re going to look at three new examples of how government intervention makes the healthcare system worse rather than better.
For our first example, let’s look at a new report from the National Center for Policy Analysis, which compares what happens when the federal government decides to build a hospital with a similar project constructed by a local government with private-sector involvement.
We’ll start with a look at Veterans Administration project.
…the VA hospital in Denver, Colorado, was run-down, crowded and outdated. …the VA considered renovating the medical facilities of the Fitzsimons Army Medical Center at a cost of $30 million. Then, the University of Colorado Hospital offered to open jointly-operated facilities for $200 million. VA officials passed on both ideas due to cost concerns. Instead, officials sought and received approval for a stand-alone facility.
That decision was very costly for taxpayers.
The VA failed to produce a design that could be built for its budget of $604 million, ultimately causing a budget-busting $1 billion overrun. …Soon, the plan to build an affordable replacement morphed into the most extravagant and expensive hospital construction project in VA history.
And, as is typical of government projects, the cost to taxpayers was far higher than initial estimates used to justify the project.
Now let’s look at another project, this one in Dallas, Texas.
…the original Parkland Hospital was built in Dallas to serve the young city’s indigent population. …its aging facilities could no longer meet the demand of 1 million patients admitted each year. …The project to rebuild Parkland, split roughly 60/40 in revenue sources, was accountable to both the public and its private donors. …Project managers hired an independent auditor to monitor all project transactions. Budget progress reports were made available to both Parkland’s Board and the public.
The final outcome was far from perfect (after all, local governments are also quite capable of wasting money). But the involvement of the private sector, combined with the fact that the local government was spending its own money, created incentives for a much better outcome.
On the first day of construction, Parkland’s project team was $100 million over budget. But a flexible design, and a willingness to balance needs and wants, allowed the team to deliver a larger, more cost-effective hospital than originally conceived for a mere 6 percent increase in budget.
And here’s a chart from the NCPA report that perfectly captures the difference between the federal government and a project involving a local government and the private sector.
Can you think of a better argument for local private-public partnerships over the federal government?
Yet policy keeps moving in the wrong direction in Washington.
The Obamacare boondoggle was all about increasing the federal government’s control and intervention in the healthcare sector.
And this brings us to our second not-so-great example of government-run healthcare.
The New York Times has a story with a real-world example showing how the President’s failed legislation is hurting small businesses.
LaRonda Hunter…envisioned…a small regional collection of salons. As her sales grew, so did her business, which now encompasses four locations — but her plans for a fifth salon are frozen, perhaps permanently.
And why can’t she expand her business and create jobs?
Because Obamacare makes it impossible.
Starting in January, the Affordable Care Act requires businesses with 50 or more full-time-equivalent employees to offer workers health insurance or face penalties that can exceed $2,000 per employee. Ms. Hunter, who has 45 employees, is determined not to cross that threshold. Paying for health insurance would wipe out her company’s profit and the five-figure salary she pays herself from it, she said.
And Ms. Hunter is just the tip of the iceberg.
For some business owners on the edge of the cutoff, the mandate is forcing them to weigh very carefully the price of growing bigger. “There’s kind of a deer-in-headlights moment for those who say, ‘I have this new potential client, but if I bring them on, I have to hire five additional people,’” said Philip P. Noftsinger, the payroll unit president at CBIZ, a financial services provider for businesses. “They’re really trying to assess how much the 50th employee is going to cost. …Added to that cost are the administrative requirements. Starting this year, all companies with 50 or more full-time workers — even those not yet required to offer health benefits — must file new tax forms with the Internal Revenue Service that provide details on employee head count and any health insurance offered. Gathering the data requires meticulous record-keeping. “These are some of the most complex informational returns we’ve ever seen,” said Roger Prince, a tax lawyer.
Here’s another real-world example.
The expense and distraction of all that paperwork is one of the biggest frustrations for one business owner, Joseph P. Sergio. …He is reluctant to go over the 50-employee line and incur all of the new rules that come with it. That makes bidding for new jobs an arduous and risky exercise. …”If you ramp up, and it pushes you over 50, there’s all these unknown costs and complicated rules. Are we really going to be able to benefit from going after that opportunity? It freezes you at a time when you need to be moving fast.”
That’s the kind of two-for-one special that’s only possible with big government!
Now that we’ve cited examples of bad policy from the Veterans Administration and Obamacare, let’s turn to Medicare for our third example.
Veronique de Rugy of the Mercatus Center writes about rampant Medicare fraud in her syndicated column.
Medicare is rife with fraud, and every year, billions of dollars are improperly paid out by the federal government’s giant health care bureaucracy. According to the government’s latest estimates, Medicare fee-for-service (parts A and B) made $46 billion in improper payments last year. And Medicare Advantage (Part C) and Medicare Prescription Drug Coverage (Part D) combined for another $15 billion in improper payments. Even more disturbing is the possibility that these numbers underestimate the annual losses to taxpayers from fraud and bureaucratic bungling. According to the work of Harvard University’s Malcolm Sparrow, fraud could account for as much as 20 percent of total federal health care spending, which would be considerably higher than what the government’s figures indicate.
But there is a glimmer of good news. There’s actually a program to identify and recover wasted funds.
The RAC program is geared toward correcting improper payments… The auditors thus pay for themselves with the money they recoup instead of simply being handed a lump-sum check. That the RAC program has an incentive to reduce wasteful spending and save taxpayers money makes it fairly unusual among government initiatives.
Unfortunately, no good deed goes unpunished in Washington.
…bureaucrats are set to greatly diminish the program’s effectiveness in 2016. Rather than empower these fraud hunters, they are drastically reducing the number of paid claims that auditors can review every 45 days (from 2 percent down to just 0.5 percent). The new limits will make it that much harder for auditors — whose cost already amounts to just a drop in the bucket — to recoup taxpayer losses.
I’ve also written about this absurd effort to curtail the RAC program, but Veronique makes a critically important observation that has widespread applicability to so much of what happens with government.
Agency failure is routinely rewarded in Washington with bigger budgets and greater authority, but here success will not be.
This, in a nutshell, is the difference between the private sector and the government.
In my speeches, I sometimes point out that people in the private economy make mistakes all the time, but I also explain that the incentive to earn profits and avoid losses creates a powerful incentive structure to quickly learn from mistakes.
That means resources quickly get reallocated in ways that are more likely to boost economic efficiency and increase growth and living standards.
In government, by contrast, this process is reversed. Bureaucrats and politicians reflexively argue that failure simply means that budgets should be expanded.
All of which explains why these cartoons are such perfect depictions of government.
Shortly after Obamacare was enacted, I started writing about groups victimized by the law. But after highlighting how children,low-income workers, andretirees were disadvantaged by government-run healthcare, I soon realized that I wasn’t saying anything new or different.
Heck, Obamacare has been such a disaster that lots of people have been writing lots of good articles about the law’s failure and how various segments of the population are being unjustly harmed.
So I chose a different approach. I decided to identify groups that deserve to suffer because of the law. Or at least to highlight slices of the population that are not very deserving of sympathy.
Now we have another group to add to this list. And this group is definitely in the deserve-to-suffer category.
That’s because we’re going to look at the big insurance companies that supported Obamacare, but now are squealing because the law isn’t working and they’re not getting the bailouts they were promised.
Here are some excerpts from a column by the irreplaceable Tim Carney of the Washington Examiner.
Until recently, the insurance giants saw Obamacare as a cash cow. They are now finding the law’s insurance marketplaces to be sickly quagmires causing billions in losses. …United Healthcare, the nation’s largest insurer, last week announced it was suffering huge losses in the exchanges. …The company forecast $700 million in losses on the exchanges. Fellow insurance giant Aetna also said it expected to lose money on the exchanges, and other insurers said enrollment was lower than they expected.
…Obamacare insiders — the wealthy and powerful operatives who alternate between top government jobs and top industry jobs — are hustling to find more bailout money for insurers. Republicans, if they are able to hold their ground in the face of lobbyist pressure, can block the bailout of Obamacare and its corporate clientele. …Obamacare included…a three-year safety net for insurers who do much worse than expected, paid for by an extra tax on insurers who do much better. The Centers for Medicare & Medicaid Services (CMS) had announced in October that insurers losses for 2014 entitled them to $2.87 billion in bailout payments… The problem is that super-profitable insurers did not pay nearly that much into the bailout fund.
This means there will be a fight in Washington. The Obama White House wants to bail out its corporate cronies. But there’s not enough money in the bailout fund.
And, thanks to Senator Rubio of Florida, the government can’t write checks out of thin air.
In late 2014, Sen. Marco Rubio, R-Fla., inserted into the so-called Cromnibus spending bill a provision that prohibited CMS from paying out more in risk corridor payments than it takes in. Profitable insurers — not taxpayers — must subsidize their less profitable peers.
CMS announced last week that the government was going to find a way to pay the insurers their full bailout, anyway. …CMS also declared the unfunded portion of Obamacare’s initial promised insurer bailout was nevertheless an “obligation of the United States Government for which full payment is required,” even though at least under the current appropriation law it is illegal.
Tim outlines the incestuous relationship between Big Insurance and the Obama White House, all of which makes for nauseating reading.
But here’s the part that matters for public policy.
Rubio’s provision…expires along with the current government funding law on December 11. The Obamacare insiders, led by Slavitt and Tavenner, will fight to free up their bailouts and put the taxpayers on the hook for their losses caused by the law they supported.
In other words, we’re about to see – as part of upcoming appropriations legislation – if Republicans have the intelligence and fortitude to retain Rubio’s anti-bailout provision.
Especially since Obamacare is still very unpopular.
But what if Obama says “boo” and threatens to veto spending legislation if it doesn’t give him carte blanche bailout authority? Will GOPers be so scared of a partial government shutdown that they instantly surrender?
After all, when there was a shutdown fight in 2013, Republicans suffered a horrible defeat in the 2014 mid-term elections. Right? Isn’t that what happened?
P.S. Let’s not forget that there is one very tiny segment of America that has unambiguously benefited from Obamacare.
P.P.S. If you have any friends who work for the corrupt health insurance companies that are worried about a potential loss of bailout money, you can cheer them up this Christmas season with some great – and very appropriate – action figure toys.
And since the law went into effect, I’ve pointed out – over and over again – the predictably negative effects of giving the government even more control.
So I’m tempted to wash my hands of the issue.
But that would be wrong, particularly since advocates of statism disingenuously might claim that silence somehow means acceptance or approval.
Moreover, we need to continuously remind ourselves that big government doesn’t work just in case there’s a chance to enact good reforms after Obama leaves office.
With that in mind, let’s look at recent developments that underscore the case against government-run healthcare.
…the GAOreportshowed that federal auditors 11 out of 12 times were able to gain subsidized coverage with fictitious applications, three of the successful applications never provided citizenship or immigration documentation. The investigators in each case were able to obtain $2,500 or around $30,000 annually in advance premium tax credits.
And what about the fact that the Obamacare co-ops have been a big flop?
Nonprofit co-ops, the health care law’s public-spirited alternative to mega-insurers, are awash in red ink and many have fallen short of sign-up goals, a government audit has found. Under President Barack Obama’s overhaul, taxpayers provided $2.4 billion in loans to get the co-ops going, but only one out of 23 — the one in Maine — made money last year, said the report out Thursday. Another one…was shut down by regulators over financial concerns. The audit by the Health and Human Services inspector general’s office also found that 13 of the 23 lagged far behind their 2014 enrollment projections.
Or what about the fact that deductibles have increased under Obamacare?
A survey released earlier this week by the Kaiser Family Foundation found that..deductibles have risen almost three times as fast since 2010 for employer-sponsored plans.
…the actuaries estimated that health spending that year jumped by 5.5 percent, a bigger rise than the country had experienced in five years. …The actuaries cited three main reasons they think health spending is set to tick up. One is the aging of the population… Another is the improving economy… But the third, and a big one, was Obamacare’s coverage expansion.
All of the aforementioned things are contrary to what Obamacare supporters promised.
Though since I focus on policy rather than politics, I’ll take this opportunity to point out that higher deductibles in some ways are a good thing. Which is why I’ve defended Obamacare’s Cadillac tax.
But now let’s look at two additional Obamacare developments. And both represent very bad news.
First, new scholarly research shows that Obamacare will be bad news for all income levels, and even will be of questionable value to those getting big subsidies (h/t: Marginal Revolution).
…the average financial burden will increase for all income levels once insured. Subsidy-eligible persons with incomes below 250 percent of the poverty threshold likely experience welfare improvements that offset the higher financial burden, depending on assumptions about risk aversion and the value of additional consumption of medical care. However, even under the most optimistic assumptions, close to half of the formerly uninsured (especially those with higher incomes) experience both higher financial burden and lower estimated welfare.
In other words, people generally were making sensible choices when they had some degree of freedom.
But now that they’re being coerced into Obamacare, many of them are worse off. Even in many cases if they’re the ones getting subsidized!
Second, we now know that President Obama’s promise to lower health insurance premiums by $2,500 was laughably misleading.
But it’s not simply that the President exaggerated. As Investor’s Business Daily explains, the numbers actually have gone in the other direction
Since 2008, average family premiums have climbed a total of $4,865. The White House cheered thenews, saying it was a sign of continued slow growth in premium costs. …Slightly less higher premiums aren’t what President Obama promised Americans when he ran for office touting his medical overhaul. He specifically said his plan would cut premiums. “We will start,” Obama said back in 2008, “by reducing premiums by as much as $2,500 per family.”
And keep in mind that Obama’s claim of big savings was not a one-time, off-the-cuff comment.
As you can see in this video, it was a pervasive part of his campaign for further government control of the health care system.
But the real story isn’t prevarication by a politician. That comes with the territory.
The real issue is that our healthcare system is more screwed up because government now is playing a bigger role.
And keep in mind that fixing the problem means a lot more than simply repealing Obamacare. We also need to deal with spending programs such asMedicare andMedicaid and address tax preferences and regulations that encourage over-insurance.
I’m a long-time advocate of “dynamic scoring,” which means I want the Congressional Budget Office and Joint Committee on Taxation to inform policy makers about how fiscal policy changes can impact overall economic performance and therefore generate “feedback” effects.
I also think the traditional approach, known as “static scoring,” creates a bias for bigger government because it falsely implies that ever-higher tax rates and an ever-growing burden of government spending don’t have any adverse impact on prosperity.
There’s a famous example to show the lunacy of static scoring. Back in late 1980s, former Oregon Senator Bob Packwood asked the Joint Committee on Taxation to estimate the revenue impact of a 100 percent tax rate on income over $200,000.
When considering such a proposal, any normal person with even the tiniest amount of common sense is going to realize that successful people quickly will figure out it makes no sense to either earn or report income about that level. As such, the government won’t collect any additional revenue.
Heck, it’s not just that the government won’t collect additional revenue. Our normal person with a bit of common sense is going to take the analysis one step further and conclude that revenues will plunge, both because the government will lose the money it collected with the old income tax rates on income above $200,000 (i.e., the income that will disappear) and also because there will be all sorts of additional economic damage because of foregone work, saving, investment, and entrepreneurship.
But the JCT apparently didn’t have any bureaucrats with a shred of common sense. Because, as shown in Part II of my video series on the Laffer Curve, they predicted that such a tax would raise $104 billion in 1989, rising to $299 billion in 1993.
The good news is that both CBO and JCT are now seeking to incorporate some dynamic scoring into their fiscal estimates. Most recently, the CBO (with help from the JCT) released a report on the fiscal impact of repealing Obamacare.
Let’s look at what they did to see whether the bureaucrats did a good job.
I’ll start with something I don’t like. This new CBO estimate is fixated on the what will happen to deficit levels.
Here’s the main chart from the report. It compares what will happen to red ink if Obamacare is repealed, based on the static score (no macro feedback) and the dynamic score (with macro feedback).
There’s nothing wrong, per se, with this type of information. But making deficits the focus of the analysis is akin to thinking that the time of possession is more important than the final score in the Super Bowl.
What matters for more is what happens to the economy, which is affected by the size and structure of government. As such, here’s the most important finding from the report.
Repeal of the ACA would raise economic output…the resulting increase in GDP is projected to average about 0.7 percent over the 2021–2025 period.
There are two reasons the bureaucrats expect better economic performance if Obamacare is repealed. First, people will have more incentive to work because of a reduction in handouts.
CBO and JCT estimate that repealing the ACA would increase the supply of labor and thus increase aggregate compensation (wages, salaries, and fringe benefits) by an amount between 0.8 percent and 0.9 percent over the 2021–2025 period. …the subsidies and tax credits for health insurance that the ACA provides to some people are phased out as their income rises—creating an implicit tax on additional earnings—and those subsidies, along with expanded eligibility for Medicaid, generally make it easier for some people to work less or to stop working.
Second, the analysis also recognizes that there would be positive economic results from repealing the tax hikes in Obamacare, especially the ones that exacerbate the tax code’s bias against saving and investment.
Implementation of the ACA is also expected to shrink the capital stock, on net, over the next decade, so a repeal would increase the capital stock and output over that period. In particular, repealing the ACA would increase incentives for capital investment, both by increasing labor supply (which makes capital more productive) and by reducing tax rates on capital income. …repealing the ACA also would eliminate several taxes that reduce people’s incentives to save and invest—most notably the 3.8 percent tax on various forms of investment income for higher-income individuals and families. The resulting increase in the incentive to save and invest—relative to current law—thus would gradually boost the capital stock; consequently, output would be higher.
And here’s the most important table from the report. And it’s important for a reason that doesn’t get sufficient attention in the report, which is the fact that repeal of Obamacare will reduce the burden of spending and the burden of taxation. I’ve circled the relevant numbers in red.
Returning to something I touched on earlier, the CBO report gives inordinate attention to the fact that there’s a projected increase in red ink because the burden of spending doesn’t fall as much as the burden of taxation.
My grousing about CBO’s deficit fixation is not just cosmetic. To the extent that the report has bad analysis, it’s because of an assumption that the deficit tail wags the economic dog.
Here’s more of CBO’s analysis.
Although the macroeconomic feedback stemming from a repeal would continue to reduce deficits after 2025, the effects would shrink over time because the increase in government borrowing resulting from the larger budget deficits would reduce private investment and thus would partially offset the other positive effects that a repeal would have on economic growth. …CBO and JCT…estimate that repealing the act ultimately would increase federal deficits—even after accounting for other macroeconomic feedback. Larger deficits would leave less money for private investment (a process sometimes called crowding out), which reduces output. …The same macroeconomic effects that would generate budgetary feedback over the 2016–2025 period also would operate farther into the future. …the growing increases in federal deficits that are projected to occur if the ACA was repealed would increasingly crowd out private investment and boost interest rates. Both of those developments would reduce private investment and thus would dampen economic growth and revenues.
Some of this is reasonable, but I think CBO is very misguided about the importance of deficit effects compared to other variables.
To give you an idea of why CBO’s deficit fixation is wrong, consider the fact that its report got a glowing review from Vox’s Matt Yglesias. Matt, you may remember, recently endorsed a top tax rate of 90 percent, so if he believes A on fiscal policy, you can generally assume the right answer is B.
Here’s some of what he wrote.
Let us now praise Keith Hall. …his CBO appointment was bound up with a push by the GOP for more “dynamic scoring” of tax policy. …Yet today Hall’s CBO released its first big dynamic score of something controversial, and it’s … perfectly sensible.
Yes, parts of the report are sensible, as I wrote above.
But Matt thinks it’s sensible because it focuses on deficits, which allows his side to downplay the negative economic impact of Obamacare.
…the ACA makes it less terrible to be poor. By making it less terrible to be poor, the ACA reduces the incentive to do an extra hour or three at an unpleasant low-wage job in order to put a little more money in your pocket. CBO’s point is that when you do this, you shrink the overall size of GDP and thus the total amount of federal tax revenue. …The change…is big enough to matter economically (tens of billions of dollars a year are at stake) but not big enough to matter for the world of political talking points where the main question is does the deficit go up or down.
Yes, you read correctly. He’s celebrating the fact that people now have less incentive to be self-reliant.
P.S. On a totally different topic, it’s time to brag about America having better policy than Germany. At least with regard to tank ownership.
I’ve previously written about legal tank ownership in the United States. But according to a BBCreport, Germans apparently don’t have this important freedom.
The Panther tank was removed from the 78-year-old’s house in the town of Heikendorf, along with a variety of other military equipment, including a torpedo and an anti-aircraft gun, Der Tagesspiegel website reports. …the army had to be called in with modern-day tanks to haul the Panther from its cellar. It took about 20 soldiers almost nine hours to extract the tank… It seems the tank’s presence wasn’t much of a secret locally. Several German media reports mention that residents had seen the man driving it around town about 30 years ago. “He was chugging around in it during the snow catastrophe in 1978,” Mayor Alexander Orth was quoted as saying.
You know what they say: If you outlaw tanks, only outlaws will have tanks.
I’m also impressed the guy had an anti-aircraft gun. The very latest is self defense!
And a torpedo as well. Criminals would have faced resistance from the land, air, and sea.
If nothing else, he must have a big house.
One that bad guys probably avoided, at least if they passed the famous IQ test for criminals and liberals.
I feel compelled to comment on the Supreme Court’s latest Obamacare decision, though I could sum up my reaction with one word: disgust.
I’m disgusted that we had politicians who decided in 2009 and 2010 to further screw up the healthcare system with Obamacare.
I’m disgusted the IRS then decided to arbitrarily change the law in order to provide subsidies to people getting insurance through the federal exchange, even though the law explicitly says those handouts were only supposed to go to those getting policies through state exchanges (as the oily Jonathan Gruber openly admitted).
I’m disgusted that the lawyers at the Justice Department and the Office of White House Counsel didn’t have the integrity to say that handouts could only be given to people using state exchanges.
But most of all, I’m disgusted that the Supreme Court once again has decided to put politics above the Constitution.
In theory, the courts play a valuable role in America’s separation-of-powers system. They supposedly protect our freedoms from majoritarianism. And they ostensibly preserve our system of checks and balances by preventing other branches of the federal government from exceeding their powers.
To be sure, the courts – including and especially the Supreme Court – have not done a good job in some areas. Ever since the 1930s, for instance, they’ve completely failed to limit the federal government to the enumerated powers in Article 1, Section 8, of the Constitution.
The Supreme Court’s first Obamacare decision back in 2012 then took that negligence to a higher level.
Now we have a second Obamacare decision. And this one may be even more outrageous because the Supreme Court decided to act as a pseudo-legislature by arbitrarily re-writing Obamacare.
The most durable damage from Thursday’s decision is not the perpetuation of the ACA, which can be undone by what created it — legislative action. The paramount injury is the court’s embrace of a duty to ratify and even facilitate lawless discretion exercised by administrative agencies and the executive branch generally. …The decision also resulted from Chief Justice John G. Roberts Jr.’s embrace of the doctrine that courts, owing vast deference to the purposes of the political branches, are obligated to do whatever is required to make a law efficient, regardless of how the law is written. What Roberts does by way of, to be polite, creative construing (Justice Antonin Scalia, dissenting, calls it “somersaults of statutory interpretation”) is legislating, not judging. …Thursday’s decision demonstrates how easily, indeed inevitably, judicial deference becomes judicial dereliction, with anticonstitutional consequences. We are, says William R. Maurer of the Institute for Justice, becoming “a country in which all the branches of government work in tandem to achieve policy outcomes, instead of checking one another to protect individual rights.
Here’s the bottom line, from Will’s perspective.
The Roberts Doctrine facilitates what has been for a century progressivism’s central objective, the overthrow of the Constitution’s architecture. The separation of powers impedes progressivism by preventing government from wielding uninhibited power.
Here’s how my Cato colleagues reacted, starting with Michael Cannon, our healthcare expert whose heroic efforts at least got the case to the Supreme Court.
…the Supreme Court allowed itself to be intimidated. …the Court rewrote ObamaCare to save it—again. In doing so, the Court has sent a dangerous message to future administrations… The Court today validated President Obama’s massive power grab, allowing him to tax, borrow, and spend $700 billion that no Congress ever authorized. This establishes a precedent that could let any president modify, amend, or suspend any enacted law at his or her whim.
Now let’s look at the responses of two of Cato’s constitutional scholars. Roger Pilon is less than impressed, explaining that the Roberts’ decision is a bizarre combination of improper deference and imprudent activism.
With Chief Justice Roberts’s opinion for the Court, therefore, we have a perverse blend of the opposing positions of the judicial restraint and activist schools that reigned a few decades ago. To a fault, the Court today is deferential to the political branches, much as conservatives in the mold of Alexander Bickel and Robert Bork urged, against the activism of the Warren and Burger Courts. But its deference manifests itself in the liberal activism of a Justice Brennan, rewriting the law to save Congress from itself. As Scalia writes, “the Court forgets that ours is a government of laws and not of men.”
And Ilya Shapiro also unloads on this horrible decision.
Chief Justice Roberts…admits, as he did three years ago in the individual-mandate case, that those challenging the administration are correct on the law. Nevertheless, again as he did before, Roberts contorts himself to eviscerate that “natural meaning” and rewrite Congress’s inartfully concocted scheme, this time such that “exchange established by the state” means “any old exchange.” Scalia rightly calls this novel interpretation “absurd.” …as Justice Scalia put it, “normal rules of interpretation seem always to yield to the overriding principle of the present Court: The Affordable Care Act must be saved.” …like three years ago, we have a horrendous bit of word play that violates all applicable canons of statutory interpretation to preserve the operation of a unpopular program that has done untold damage to the economy and health care system.
Now I’ll add my two cents, at least above and beyond expressing disgust. But I won’t comment on the legal issues since that’s not my area of expertise.
Instead I’ll have a semi-optimistic spin. I wrote in 2013 that we should be optimistic about repealing Obamacare and fixing the government-caused dysfunctionalism (I don’t think that’s a word, but it nonetheless seems appropriate) of our healthcare system.
This latest decision from the Supreme Court, while disappointing, doesn’t change a single word of what I wrote two years ago.
P.S. Since today’s topic (other than my conclusion) was very depressing, let’s close by looking at something cheerful.
Well, now we have further evidence. Here’s some polling data from AEI’s most recent Political Report. As you can see, there’s a much stronger belief in self-sufficiency in the United States than there is in either Germany or Italy.
In other words, just about everything we were told was a fib. Even the tiny slivers of good news resulting from Obamacare were based on falsehoods.
So I almost feel like I’m guilty of piling on by writing about another big Obamacare lie.
But Charles Krauthammer has such a strong critique of Obamacare’s mandate for electronic health records that I can’t resist. He starts by pointing out that doctors are unhappy about this costly new mandate.
…there was an undercurrent of deep disappointment, almost demoralization, with what medical practice had become. The complaint was not financial but vocational — an incessant interference with their work, a deep erosion of their autonomy and authority…topped by an electronic health records (EHR) mandate that produces nothing more than “billing and legal documents” — and degraded medicine.
Not just unhappy. Some of them are quitting and most of them are spending less time practicing actual health care.
Virtually every doctor and doctors’ group I speak to cites the same litany, with particular bitterness about the EHR mandate. As another classmate wrote, “The introduction of the electronic medical record into our office has created so much more need for documentation that I can only see about three-quarters of the patients I could before, and has prompted me to seriously consider leaving for the first time.” …think about the extraordinary loss to society — and maybe to you, one day — of driving away 40 years of irreplaceable clinical experience.
Then Krauthammer exposes the deceptions we were fed when Obamacare was being debated.
The newly elected Barack Obamatold the nation in 2009that “it just won’t save billions of dollars” — $77 billion a year,promised the administration —“and thousands of jobs, it will save lives.” He then threwa cool $27 billionat going paperless by 2015. It’s 2015 and what have we achieved? The $27 billion is gone, of course. The $77 billion in savings became a joke. Indeed, reported the Health and Human Servicesinspector general in 2014, “EHR technology can make it easier to commit fraud,” as in Medicare fraud, the copy-and-paste function allowing the instant filling of vast data fields, facilitating billing inflation.
A boondoggle on the back of taxpayers. Flushing $27 billion is bad enough, but the indirect costs also are large.
That’s just the beginning of the losses. Consider the myriad small practices that, facing ruinous transition costs in equipment, software, training and time, have closed shop, gone bankrupt or been swallowed by some larger entity. …One study in the American Journal of Emergency Medicine found that emergency-room doctorsspend 43 percent of their timeentering electronic records information, 28 percent with patients. Another study found that family-practice physiciansspend on average 48 minutes a dayjust entering clinical data.
Here’s the bottom line.
EHR is health care’s Solyndra. Many, no doubt, feasted nicely on the $27 billion, but the rest is waste: money squandered, patients neglected, good physicians demoralized.
Not much ambiguity in that sentence. To put it bluntly, “EHR” is the kind of answer you get when you ask a very silly question.
Now, thanks to Reason, we can read with envy about another elitist benefit for that gilded class.
…a little-known California state program designed to protect police and judges from the public disclosure of their home addresses had expanded into a massive database of 1.5 million public employees and their family members… Because of this Confidential Records Program, “Vehicles with protected license plates can run through dozens of intersections controlled by red light cameras and breeze along the 91 toll lanes with impunity,” according to the Orange County Register report. They evade parking citations and even get out of speeding tickets because police officers realize “the drivers are ‘one of their own’ or related to someone who is.”
You may be thinking that the law surely was changed after it was exposed by the media.
And you would be right. But if you thought the law would be changed to cut back on this elitist privilege, you would be wrong.
…the legislature did worse than nothing. It killed a measure to force these plate holders to provide their work addresses for the purpose of citations — and expanded the categories of government workers who qualify for special protections. This session, the legislature has decided to expand that list again, never mind the consequences on local tax revenues, safety and fairness. …Given the overwhelming support from legislators, expect more categories to be added to the Confidential Records Program — and more public employees and their families being free to ignore some laws the rest of us must follow.
This is such a depressing story that I’ll close today with this bit of humor about bureaucracy in the Golden State.
In the grand scheme of things, the most important development in health policy is the pending Supreme Court case revolving around whether subsidies can be provided to people obtaining health insurance from the federal exchange, even though the law explicitly says handouts are only available to people getting policies via state exchanges.
If the Court rules correctly (unlike, ahem, the last time the Justices dealt with Obamacare), it will then be very important that congressional reformers use the resulting mess to unwind as much of the law as possible.
That will be a challenge because statists already are arguing that the “only” solution is to re-write the law so that subsidies are also available via the federal government. For what it’s worth, my colleague Michael Cannon outlines the right strategy in Cato’s newly released Policy Priorities for the 114th Congress.
But let’s set aside that issue because we have a great opportunity to review another example of how government-run healthcare is a miserable failure.
Our topic for today is government-dictated electronic health records (EHRs). Dr. Jeffrey Singer is on the front lines of this issue. As a physician in Arizona, he deals with the real-world impact of this particular mandate.
And he’s so unhappy that he wrote a column on the topic for the Wall Street Journal.
Starting this year, physicians like myself who treat Medicare patients must adopt electronic health records, known as EHRs, which are digital versions of a patient’s paper charts. …I am an unwilling participant in this program. In my experience, EHRs harm patients more than they help.
By way of background, he explains that EHRs were part of Obama’s failed “stimulus” legislation and they were imposed on the theory that supposed experts could then use the resulting data to make the system more efficient and effective.
The federal government mandated in the 2009 stimulus bill that all medical providers that accept Medicare adopt the records by 2015. Bureaucrats and politicians argued that EHRs would facilitate “evidence-based medicine,” thereby improving the quality of care for patients.
But Dr. Singer says the real-world impact is to make medical care less effective and more expensive.
Electronic health records are contributing to two major problems: lower quality of care and higher costs. The former is evident in the attention-dividing nature of electronic health records. They force me to physically turn my attention away from patients and toward a computer screen—a shift from individual care to IT compliance. …The problem is so widespread that the American Medical Association—a prominent supporter of the electronic-health-record program—felt compelled to defend EHRs in a 2013report, implying that any negative experiences were the fault of bedside manner rather than the program. Apparently our poor bedside manner is a national crisis, judging by how my fellow physicians feel about the EHR program.A 2014 surveyby the industry group Medical Economics discovered that 67% of doctors are “dissatisfied with [EHR] functionality.” Three of four physicians said electronic health records “do not save them time,” according to Deloitte. Doctors reported spending—or more accurately, wasting—an average of 48 minutes each day dealing with this system.
Here’s what he wrote about costs.
The Deloitte survey also found that three of four physicians think electronic health records “increase costs.” There are three reasons. First, physicians can no longer see as many patients as they once did. Doctors must then charge higher prices for the fewer patients they see. This is also true for EHRs’ high implementation costs—the second culprit. A Novemberreportfrom the Agency for Healthcare Research and Quality found that the average five-physician primary-care practice would spend $162,000 to implement the system, followed by $85,000 in first-year maintenance costs. Like any business, physicians pass these costs along to their customers—patients. Then there’s the third cause: Small private practices often find it difficult to pay such sums, so they increasingly turn to hospitals for relief. In recent years, hospitals have purchased swaths of independent and physician-owned practices, which accounted for two-thirds of medical practices a decade ago but only half today. Two studies in the Journal of the American Medical Association and one in Health Affairs published in 2014 found that, in the words of the latter, this “vertical integration” leads to “higher hospital prices and spending.”
Last but not least, Dr. Singer explains that electronic health records don’t reduce errors or increase efficiency, notwithstanding the claims of advocates.
The EHR system assumes that the patient in front of me is the “average patient.” When I’m in the treatment room, I must fill out a template to demonstrate to the federal government that I made “meaningful use” of the system. This rigidity inhibits my ability to tailor my questions and treatment to my patient’s actual medical needs. It promotes tunnel vision in which physicians become so focused on complying with the EHR work sheet that they surrender a degree of critical thinking and medical investigation. Not surprisingly, a recent study in Perspectives in Health Information Management found that electronic health records encourage errors that can “endanger patient safety or decrease the quality of care.” America saw a real-life example during the recent Ebola crisis, when “patient zero” in Dallas, Thomas Eric Duncan, received a delayed diagnosis due in part to problems with EHRs.
Wow, not exactly an uplifting read.
Indeed, Dr. Singer’s perspective is so depressing that I hope he’s at least partially wrong. Maybe after a couple of years, and with a bit of luck, doctors will adapt and we’ll get some benefits in exchange for the $20 billion-plus of taxpayer money that has been plowed into this project (not to mention all the time and expense imposed on the medical profession).
But the big-picture lesson to be learned is that planners, politicians, and bureaucrats in Washington should not be in charge of the healthcare system.
Which brings us to the real challenge of how to put the toothpaste back in the tube.
Government intervention is so pervasive in the healthcare sector that – with a few rare exceptions – normal market forces have been crippled.
Amazingly, the statists then argue that more government is the only solution to this government-caused mess. Sort of Mitchell’s Law on steroids.
But that path leads to single-payer healthcare, and the horror stories from the U.K. should be enough to show any sensible person that’s a bad outcome.
Way back in 2010, immediately after Obamacare was rammed down our throats, I put together four guiding principles for a counter-offensive.
One of my goals was to help people understand that the problem was far greater than Obamacare. Indeed, the so-called Affordable Care Act was merely another step on a long (and very bad) journey to healthcare statism.
The way to think of Obamacare is that we are shifting from a healthcare system 68 percent controlled/directed by government to one that (when all the bad policies are phased in) is 79 percent controlled/directed by government. Those numbers are just vague estimates, to be sure, but they underscore why Obamacare is just a continuation of a terrible trend, not a profound paradigm shift.
Two years ago, I elaborated on this thesis and even put together a couple of charts to emphasize the point.
Obamacare was enacted in 2010, and it was perceived to be a paradigm-shifting change in the healthcare system, even though it was just another layer of bad policy on top of lots of other bad policy. Immediately after the legislation was approved,I offered a rough estimatethat we went from a system that was 68 percent dictated by government to one that was 79 percent dictated by government. …all of the same problems still exist, but now they’re exacerbated by the mistakes in Obamacare.
My numbers were just vague approximations, of course, but I think the basic premise was spot on.
And my theory is still accurate. But you don’t have to believe me.
Writing for the Washington Examiner, Philip Klein makes the critical point that repealing Obamacare wouldn’t result in a free-market system.
Instead, we’d be stuck with the pre-Obamacare system that was decrepit because of already-existing programs, mandates, regulations, and other forms of intervention.
…repeal is not enough. Even if simple repeal were politically obtainable, Americans would still be left with a broken healthcare system. Government regulations would still be stifling competition and individual choice and government healthcare programs would still be driving the nation’s unsustainable long-term debt problem. If Republicans achieved repeal without agreeing on a way to reform healthcare along free market lines, it’s inevitable that Democrats would eventually lead another overhaul of the system that would grant even more power to the federal government.
Philip is totally correct.
Before Obamacare, we had a system that didn’t work very well because of government. But in a horrifying example of Mitchell’s Law, many people decided that more government was the solution to the problems already caused by government.
Hence, we got so mis-named Affordable Care Act.
But if Obamacare is repealed, we’ll simply be back in the same unstable situation. And Philip is right that the statists will then simply argued for a different type of government expansion. Probably single payer, notwithstanding all the horror stories from places such as the United Kingdom.
Some may argue at this point that it doesn’t really matter because Obama is in the White House with a veto pen, so critics have a couple of years to figure out their next step.
Maybe, but it’s also possible that the Supreme Court will (for a change of pace) make the right ruling on a key Obamacare case later this year. And this would probably force policy makers to re-open the law.
…a Supreme Court decision expected by late June could invalidate Obamacare subsidies for millions of Americans. If Republicans don’t have an alternative ready, congressional leaders will be under tremendous pressure to pass a simple “fix” that would allow the subsidies to continue to flow, thus further entrenching Obamacare before a Republican president theoretically is able to act in 2017. For these reasons and many others it’s important for Republicans to unite around an alternative to Obamacare.
Philip (who has an entire book on this issue) then proceeds to categorize Obamacare critics as being in three different camps on the issue of how to proceed.
The first approach comes from those who believe that fully repealing Obamacare is probably unrealistic, but who still see an opening to reform the overall healthcare system in a more market-oriented direction. I call this the Reform School. The second approach comes from a crowd that believes full repeal is a necessity, but can only occur if opponents of the law create a market-friendly alternative with enough financial assistance to make health insurance widely available to those Americans who want to purchase it. I call this the Replace School. And finally, there is a third approach, which advocates repealing the law, returning to pre-Obamacare levels of taxes and spending, and then using that clean slate as the basis to overhaul the system in a free market manner to bring down costs. I call this the Restart School.
Since I focus on fiscal policy issues rather than healthcare, I don’t know if there are substantive – or merely strategic – differences among these three groups.
But I will say (assuming you actually want to solve the problem) that at some point you have to deal with the government programs and interventions that have given us a third-party payer crisis.
So I will reiterate what I wrote back in 2010 as part of my proposed counter-offensive.
The only way to fix healthcare is to restore the free market. That means going back to a system where people pay out-of-pocket for most healthcare and use insurance to protect against genuine risk and catastrophic expenses. The time has come to reduce the size and scope of government. …Change Medicare into a system based on personal health accounts and shift all means-tested spending to the states. …the flat tax is ideal from a healthcare perspective since it gets rid of the healthcare exclusion in the tax code as part of a shift to a tax system with low rates and no double taxation.
This video, narrated by Julie Borowski for the Center for Freedom and Prosperity, looks at the Obamacare/third-party payer issue.
And if you want to examine some of the component issues of healthcare reform, we have videos on Medicaid, Medicare, and tax reform.
One of the good things about working at the Cato Institute is that there’s never any pressure to put your thumb on the scale to help any political party.
Our loyalties are to libertarian principles, many of which are reflected in the Constitution, so we’re free to criticize or praise politicians based on their ideas rather than their partisan affiliation.
I’m giving this background because today I’m going to say something nice about Obamacare.
Not because I like the overall law, but because honesty is the best policy.
Regular readers know that our healthcare system is screwed up by bad government policy. More specifically, spending programs such as Medicare and Medicaid, combined with tax preferences and regulations that encourage over-insurance, have created a giant third-party payer problem.
Only 11 percent of health care spending in America is directly financed by consumers. The rest is paid for by taxpayers, insurance companies, and other third parties.
This has eviscerated the normal working of a competitive market. When people are spending their own money, they are careful and prudent. When they spend other people’s money, however, they are not overly concerned about cost.
As a result, we have a needlessly expensive system. And because third-party payer requires lots of administration and paper work, bad government policies also have caused absurd levels of inefficiency.
Well, there’s one small piece of Obamacare that actually is helping to mitigate this problem. The law includes a so-called Cadillac tax that caps the special tax preference for fringe benefits (if your employer provides you a health insurance policy as part of your compensation, that type of income isn’t taxed, unlike your cash wages).
And that reform is having a positive impact. Here are some passages from a Bloombergstory.
Large employers are increasingly putting an end to their most generous health-care coverage as a tax on “Cadillac” insurance plans looms closer under Obamacare. Employees including bankers atJPMorgan Chase & Co. (JPM)and college professors atHarvard Universityare seeing a range of moves to shift more costs to workers. …The tax takes effect in 2018, and employers are already laying the groundwork to make sure they don’t have to pay the 40 percent surcharge on health-insurance spending that exceeds $27,500 for a family or $10,200 for an individual. Once envisioned as a tool to slow the nation’s growing health-care tab, the tax has in practice meant higher out-of-pocket health-care costs for workers.
The last sentence in the excerpt, by the way, is economically illiterate.
The Cadillac tax will restrain health spending because it means higher out-of-pocket costs for consumers. They are going to have more authority and responsibility of how to spend their own money.
Think of this analogy. Will you eat more if I give you $25 to buy a meal or if I give you a pre-paid voucher for a $25 all-you-can-eat buffet?
If you’re a normal person, you’ll take the $25 cash, buy a meal for less than that amount, and save the extra money for something else.
But if you’re given a pre-paid voucher for the buffet, you’ll pig out because there’s no additional cost for consuming more items.
And the Bloomberg story includes evidence that giving consumers more control over their income is having the predicted positive effect.
The tax on Cadillac plans — named after the luxury vehicle to denote their lavishness — is one reason the growth in health-care premiums has slowed since the Patient Protection and Affordable Care Act took effect in 2010. …The tax “is having the effect that was intended, which is the cost of these plans are being reduced,” Christopher Condeluci, a former Senate Republican aide who helped design it, said in a phone interview. …Premium increases for employer-provided health insurance, which covers about48 percentof Americans, “slowed markedly” in 31 states since 2010, the year the Affordable Care Act became law, the New York-based Commonwealth Fundreportedtoday. Nationally, premium growth fell by about a percentage point after the law, to 4.1 percent a year on average, the report said.
By the way, I should hasten to add that I’m not happy about the way the Cadillac tax was adopted, for a major reason and a minor reason.
The major reason is that it was part of a law that is otherwise a very expensivedisaster.
The minor reason is that, for reasons of both good tax policy and good health policy, I want to eliminate loopholes and tax preferences only if we can use every penny of revenue to finance lower tax rates.
And that’s exactly what you get with a flat tax, which is a system where you don’t even need a Cadillac tax because there’s no healthcare exclusion.
Under Obamacare, by contrast, the Cadillac tax limits the healthcare exclusion, but politicians used the money to finance bigger government.
Now let’s say something bad about Obamacare.
John Goodman of the Independent Institute has a column in today’s Wall Street Journal. He points out that the law is hurting many of the people it was supposed to help.
…the law is already hurting some of the people it was intended to help. By this time next year, we may find that many workers who earn within a few dollars of the minimum wage have less income and less insurance coverage (as a group) than they did before the mandate began to take effect.
How does John justify these assertions?
Because he did some real-world research, surveying 136 fast-food restaurants with 3,500 employees.
The results are not encouraging, at least for the workers.
Before 2014 about half the employees were “full time” as defined by ObamaCare; that is, they worked 30 hours or more a week. The potential cost to the employers of providing mandated health insurance to their full-time staff would have been about $7 million a year. But by the time the employers took advantage of all their legal options they were able to reduce their cost to less than 1% of that amount. The first step was to make all hourly workers part time. …workers in the survey whose hours were reduced to part time…can get subsidized insurance through an exchange, but they will be asked to pay up to 9.5% of their income for what is unattractive coverage. Some of them previously had mini-med plans, but this kind of insurance is no longer available to them. …Those few remaining full-time employees will get mini-med insurance for themselves, but they are unlikely to be able to afford coverage for any dependents they have. They will not get an ObamaCare bronze plan unless they fork over about one-tenth of their take-home pay, and they won’t be able to get bronze coverage for other family members unless they forfeit more than half their income. Out of 3,500 employees, only one that we know of got the kind of insurance that the architects of the Affordable Care Act wanted everyone to have.
One out of 3,500? Sounds like the typical success rate for a government program.
The bottom line is that an overwhelming percentage of Obamacare provisions make the healthcare system more expensive and less effective.
Yes, there are some positive effects of the Cadillac tax, but those are easily offset by all the features of the law that increase the size and scope of government.
P.P.S. The folks at Reason TV put together a must-watch video on how a hospital can be more efficient and affordable in the absence of third-party payer.
But since I obviously don’t control Republicans and since I freely admit that economists are lousy forecasters, let’s do something more practical to start 2015.
Let’s simply look at three very important things that may happen this year and what they might mean.
1. Will the Republican Senate support genuine entitlement reform?
One of the best things to happen in recent years is that House Republicans embraced genuine entitlement reform. For the past four years, they have approved budget resolutions that assumed well-designed structural changes to both Medicare and Medicaid.
There were no real changes in policy, of course, because the Senate was controlled by Harry Reid. And I’m not expecting any meaningful reforms in 2015 or 2016 because Obama has a veto pen.
But if the Republican-controlled Senate later this year approves a budget resolution with the right kind of Medicare and Medicaid reform, that would send a very positive signal.
I don’t even care if the House and Senate have a conference committee and proceed with actual legislation. As I noted above, Obama would use his veto pen to block anything good from becoming law anyhow.
My bottom line is simple. If GOPers in both the House and Senate officially embrace the right kind of entitlement reform, then all that’s needed is a decent President after the 2016 elections (which, of course, presents an entirely different challenge).
2. Will there be another fiscal crisis in Greece (and perhaps elsewhere in Europe)?
The European fiscal crisis has not gone away. Yes, a few governments have actually been forced to cut spending, but they’ve also raised taxes and hindered the ability of the private sector to generate economic recovery.
And the spending cuts in most cases haven’t been sufficient to balance budgets, so debt continues to grow (in some cases, there have been dramatic increases in general government net liabilities).
Sounds like a recipe for further crisis, right? Yes and no.
Yes, there should be more crisis because debt levels today are higher than they were five years ago. But no, there hasn’t been more crisis because direct bailouts (by the IMF) and indirect bailouts (by the ECB) have propped up the fiscal regimes of various European nations.
At some point, though, won’t this house of cards collapse? Perhaps triggered by election victories for anti-establishment parties (such as Syriza in Greece or Podemos in Spain)?
While I’m leery of making predictions, at some point I assume there will be an implosion.
Or might turmoil lead to good policy, which both politicians and voters sobering up and realizing that there must be limits on the overall burden of government spending?
3. If the Supreme Court rules correctly in King v. Burwell, will federal and state lawmakers react correctly?
The Supreme Court has agreed to decide a very important case about whether Obamacare subsidies are available to people who get policies from a federal exchange.
Since the law explicitly states that subsidies are only available through state exchanges (as one of the law’s designers openly admitted), it seems like this should be a slam-dunk decision.
But given what happened back in 2012, when Chief Justice Roberts put politics above the Constitution, it’s anybody’s guess what will happen with King v Burwell.
Just for the sake of argument, however, let’s assume the Supreme Court decides the case correctly. That would mean a quick end to Obamacare subsidies in the dozens of states that refused to set up exchanges.
Sounds like a victory, right?
I surely hope so, but I’m worried that politicians in Washington might then decide to amend the law to officially extend subsidies to policies purchased through a federal exchange. Or politicians in state capitals may decide to set up exchanges so that their citizens can stay attached to the public teat.
In other words, a proper decision by the Supreme Court would only be a good outcome if national and state lawmakers used it as a springboard to push for repeal of the remaining parts of Obamacare.
If, on the other hand, a good decision leads to bad changes, then there will be zero progress. Indeed, it would be a big psychological defeat since it would represent a triumph of handouts over reform.
I guess I’m vaguely optimistic that good things will happen simply because we’ve already seen lots of states turn down “free” federal money to expand Medicaid.
P.S. Let’s close with some unexpected praise for Thomas Piketty. I’m generally not a fan of Monsieur Piketty since his policies would cripple growth (hurting poor people, along with everyone else).
But let’s now look at what France 24 is reporting.
France’s influential economist Thomas Piketty, author of “Capital in the 21st Century”, on Thursday refused to accept the country’s highest award, the Legion d’honneur… “I refuse this nomination because I do not think it is the government’s role to decide who is honourable,” Piketty told AFP.
It’s quite possible, perhaps even likely, that Piketty is merely posturing. But I heartily applaud his statement about the role of government.
But let’s not lose sight of the fact that Piketty is still a crank. His supposedly path-breaking research is based on a theory that is so nonsensical that it has the support of only about 3 percent of economists.
Exactly one year ago, we looked at the best and worst policy developments of 2013.
Now it’s time for a look back at 2014 to see what’s worth celebrating and what are reasons for despair.
Here’s the good news for 2014.
1. Gridlock – I’ve been arguing for nearly three years that divided government is producing better economic performance. To be sure, it would have been difficult for the economy to move in the wrong direction after the stagnation of Obama’s first two years, but heading in the wrong direction at a slower pace is better than speeding toward European-style statism.
Indeed, the fact that policy stopped getting worse even boosted America’s relative competitiveness, so there’s a lot to be thankful for when politicians disagree with each other and can’t enact new laws.
David Harsanyi explains the glory of gridlock for The Federalist.
Gross domestic product grew by a healthy 5 percent in the third quarter, the strongest growth we’ve seen since 2003. Consumer spending looks like it’s going to be strong in 2015, unemployment numbers have looked good, buying power is up and the stock market closed at 18,000 for the first time ever. All good things. So what happened? …the predominant agenda of Washington was doing nothing. It was only when the tinkering and superfluous stimulus spending wound down that fortunes began to turn around. …spending as a percent of GDP has gone down. In 2009, 125 bills were enacted into law. In 2010, 258. After that, Congress, year by year, became one of the least productive in history. And the more unproductive Washington became, the more the economy began to improve. …Gridlock has caused an odd, but pervasive, stability in Washington. Spending has been static. No jarring reforms have passed — no cap-and-trade, which would have artificially spiked energy prices and undercut the growth we’re now experiencing. The inadvertent, but reigning, policy over the past four years has been, do no harm.
Amen. Though I should hasten to add that while gridlock has been helpful in the short run (stopping Obama from achieving his dream of becoming a second FDR), at some point we will need unified government in order to adopt much-needed tax reform and entitlement reform.
The key question is whether we will ever get good politicians controlling both ends of Pennsylvania Avenue.
2. Restrained Spending – This is the most under-reported and under-celebrated news of the past few years, not just 2014.
In fiscal year 2009, the federal government spent about $3.52 trillion. In fiscal year 2014 (which ended on September 30), the federal government spent about $3.50 trillion. In other words, there’s been no growth in nominal government spending over the past five years. It hasn’t received nearly as much attention as it deserves, but there’s been a spending freeze in Washington. …the fiscal restraint over the past five years has resulted ina bigger drop in the relative size of governmentin America than what Switzerland achieved over the past ten years thanks to the “debt brake.” …The bottom line is that the past five years have been a victory for advocates of limited government.
And this spending restraint is producing economic dividends, though Paul Krugman somehow wants people to believe that Keynesian economics deserves the credit.
3. Limits on Unemployment Benefits – Although the labor force participation rate is still disturbingly low, the unemployment rate has declined and job creation numbers have improved.
The aforementioned policies surely deserve some of the credit, but it’s also worth noting that Congress wisely put a stop to the initiative-sapping policy of endlessly extending unemployment benefits. Such policies sound compassionate, but they basically pay people not to work and cause more joblessness.
Phil Kerpen of American Commitment elaborates, citing recent research from the New York Fed.
According to empirical researchby the Federal Reserve Bank of New York: “most of the persistent increase in unemployment during the Great Recession can be accounted for by the unprecedented extensions of unemployment benefit eligibility.” Those benefits finally ended at the end of 2013, triggering a sharp rise in hiring… Specifically, they found that the average extended unemployment benefits duration of 82.5 weeks for four years had the impact of raising the unemployment rate from 5 percent to 8.6 percent. …Good intentions are not enough in public policy. It might seem kind and compassionate to spend billions of taxpayer dollars on “emergency” unemployment benefits forever, but the effect is to keep millions of people unemployed. Results matter.
Phil’s right. If you pay people not to work, you’re going to get foolish results.
But the three above stories are not the only rays of sunshine in 2014. Honorable mention goes to North Carolina and Kansas for implementing pro-growth tax reforms.
I’m also pleased that GOPers passed the first half of my test and told the Democrat appointee at the Congressional Budget Office that he would be replaced. Now the question is whether they appoint someone who will make the long-overdue changes that are needed to get better and more accurate assessments of fiscal policy. That didn’t happen when the GOP had control between 1995 and 2007, so victory is far from assured.
And another honorable mention is that Congress has not expanded the IMF’s bailout authority.
Now let’s look at the three worst policy developments of 2014.
1. Obamacare Subsidies – Yes, Obamacare has been a giant albatross for the President and his party. Yes, the law has helped more and more people realize that big government isn’t a good idea. Those are positive developments.
Nonetheless, 2014 was the year when the subsidies began to flow. And once handouts begin, politicians get very squeamish about taking them away.
This is why I wrote back in 2012 that Obamacare may have been a victory (in the long run) for the left, even though it caused dozens of Democrats to lose their seats in the House and Senate.
I think the left made a clever calculation that losses in the last cycle would be an acceptable price to get more people dependent on the federal government. And once people have to rely on government for something like healthcare, they are more likely to vote for the party that promises to make government bigger. …This is why Obamacare – and the rest of the entitlement state – is so worrisome. If more and more Americans decide to ride in the wagon of government dependency, it will be less and less likely that those people will vote for candidates who want to restrain government.
Simply stated, when more and more people get hooked on the heroin of government dependency, I fear you get the result portrayed in this set of cartoons.
2. Continuing Erosion of Tax Competition – Regular readers know that I view jurisdictional competition as a very valuable constraint on the greed of the political class.
Simply stated, politicians will be less likely to impose punitive tax policies if the geese with the golden eggs can fly away. That’s why I cheer when taxpayers escape high-tax jurisdictions, whether we’re looking at New Jersey and California, or France and the United States.
But this also helps to explain why governments, either unilaterally or multilaterally, are trying to prevent taxpayers from shifting economic activity to low-tax jurisdictions.
Here’s an example, from the Wall Street Journal, of politicians treating taxpayers like captive serfs.
Japan could become the latest country to consider taxing wealthy individuals who move abroad to take advantage of lower rates. The government and ruling party lawmakersare considering an “exit tax”… Such a rule would prevent wealthy individuals moving to a location where taxes are low–such as Singapore or Hong Kong… some expats in Tokyo are concerned the rule could make companies think twice about sending senior professionals to Japan or make Japanese entrepreneurs more reluctant to go abroad.
My reaction, for what it’s worth, is that Japan should reduce tax rates if it wants to keep people (and their money) from emigrating.
3. Repeating the Mistakes that Caused the Housing Crisis – A corrupt system of subsidies for Fannie Mae and Freddie Mac, combined with other misguided policies from Washington, backfired with a housing bubble and financial crisis in 2008.
Inexplicably, the crowd in Washington has learned nothing from that disaster. New regulations are being proposed to once again provide big subsidies that will destabilize the housing market.
Peter Wallison of the American Enterprise Institute warns that politicians are planting the seeds for another mess.
New standards were supposed to raise the quality of the “prime” mortgages that get packaged and sold to investors; instead, they will have the opposite effect. …the standards have been watered down. …The regulators believe that lower underwriting standards promote homeownership and make mortgages and homes more affordable. The facts, however, show that the opposite is true. …low underwriting standards — especially low down payments — drive housing prices up, making them less affordable for low- and moderate-income buyers, while also inducing would-be homeowners to take more risk. That’s why homes were more affordable before the 1990s than they are today. … The losers, as we saw in the financial crisis, are borrowers of modest means who are lured into financing arrangements they can’t afford. When the result is foreclosure and eviction, one of the central goals of homeownership — building equity — is undone.
Gee, it’s almost as if Chuck Asay had perfect foresight when drawing this cartoon.
Let’s end today’s post with a few dishonorable mentions.
In addition to the three developments we just discussed, I’m also very worried about the ever-growing red tape burden. This is a hidden tax that undermines economic efficiency and enables cronyism.
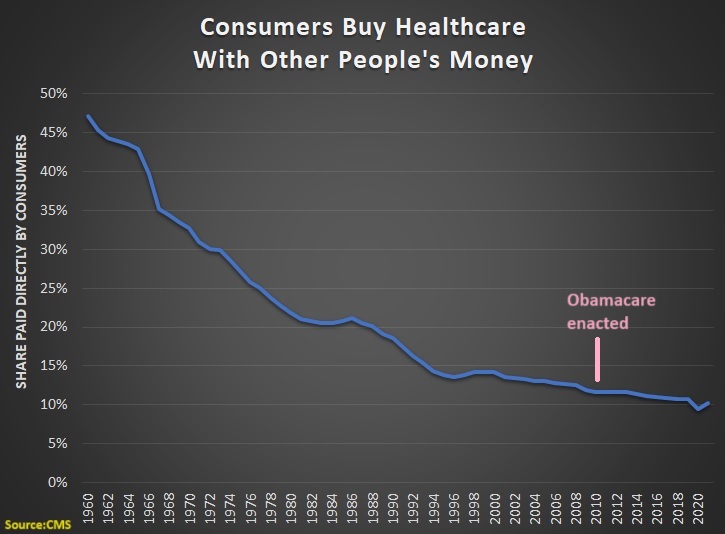
All these years later, we still haven’t found the magic money pot. …Obamacare contained a lot of elements that were expected to realize significant cost savings while actually improving the quality of care. …What this demonstrates is how hard it is to actually change the system in ways that generate major savings. …the wonks hunting for magic pots of money have mostly turned out to be chasing rainbows.

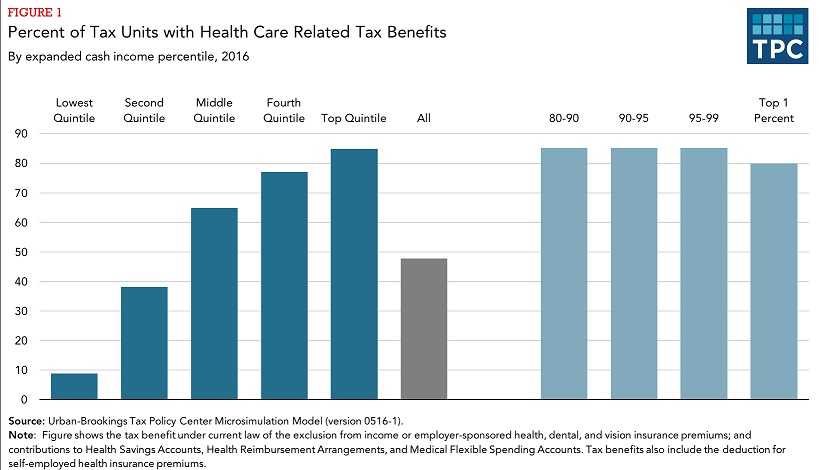














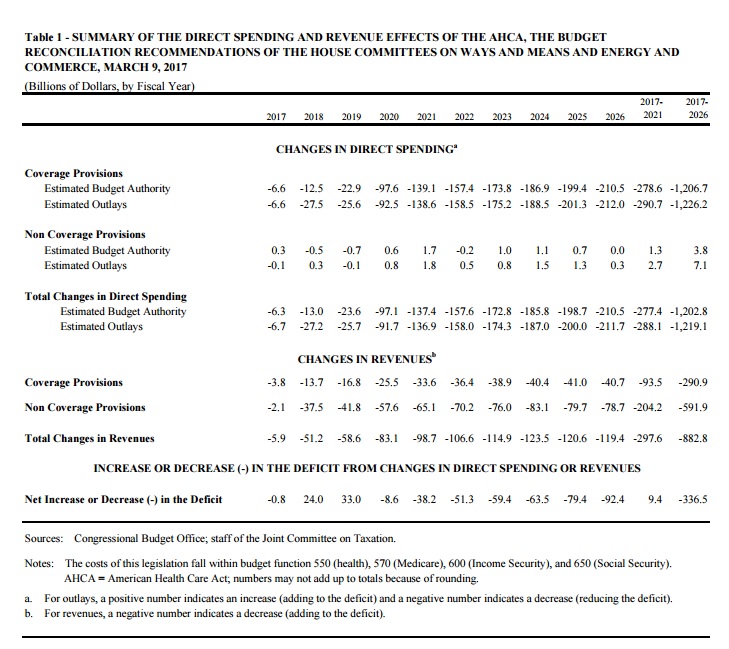


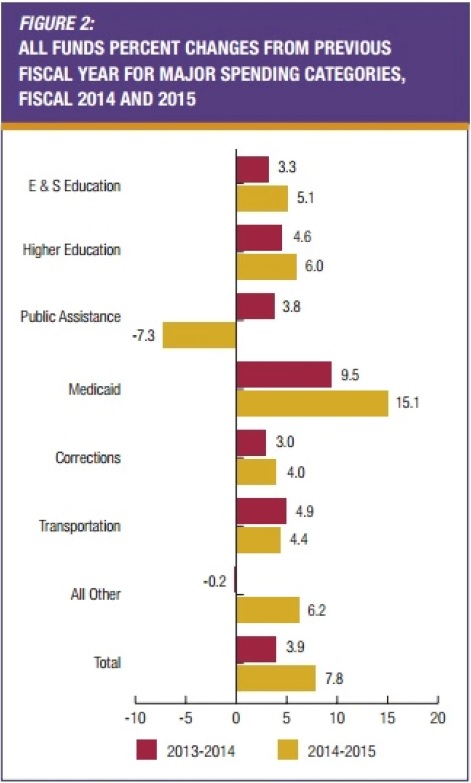

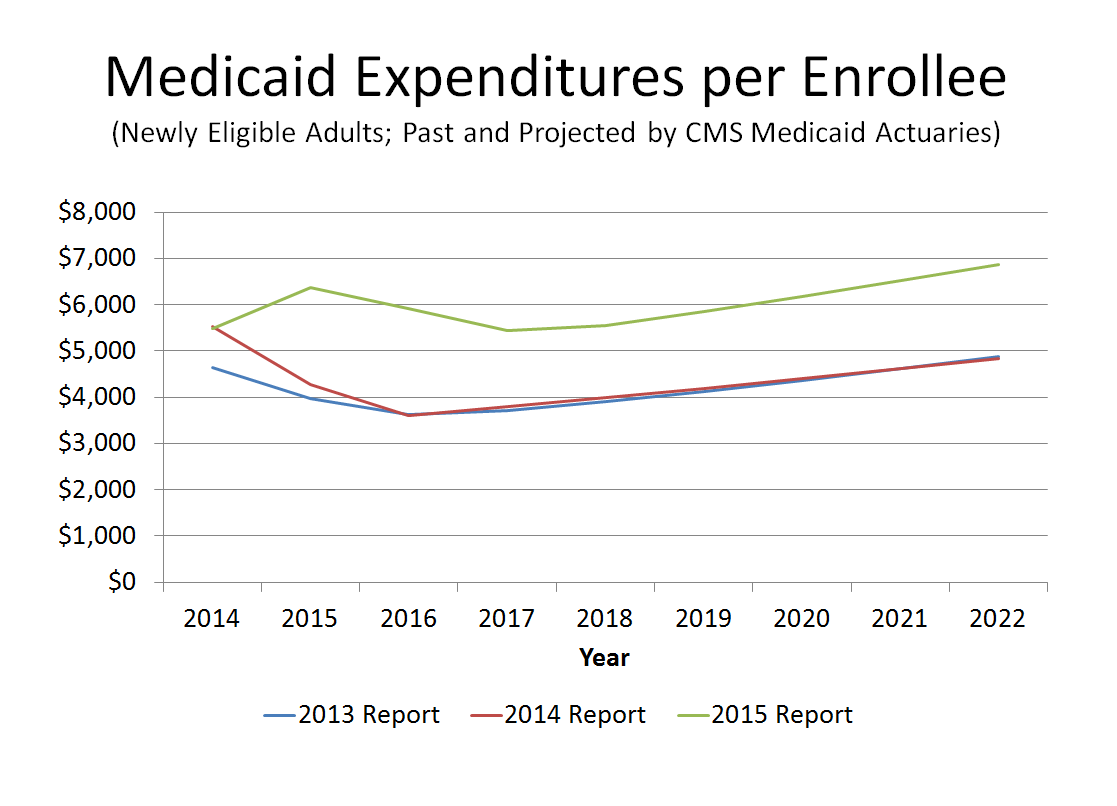

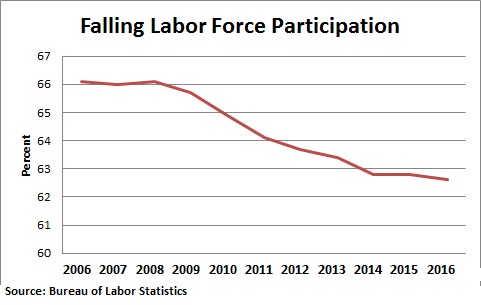








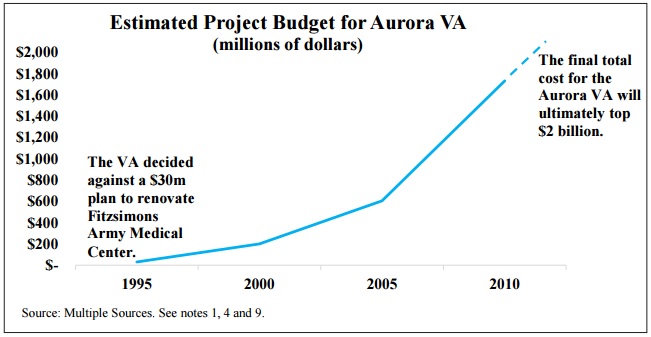
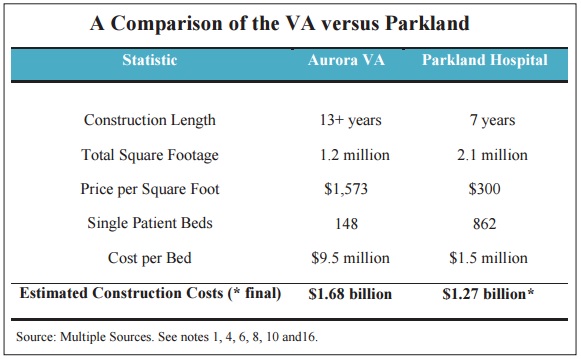





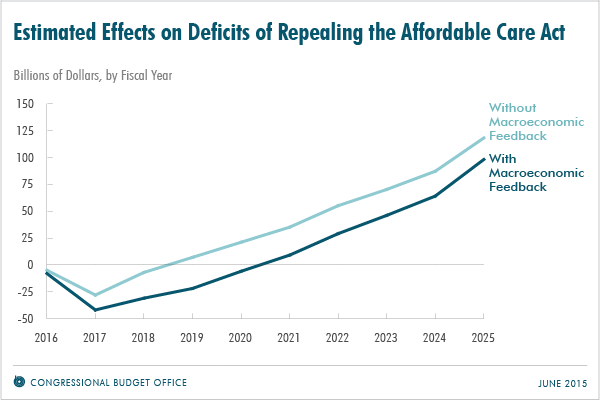
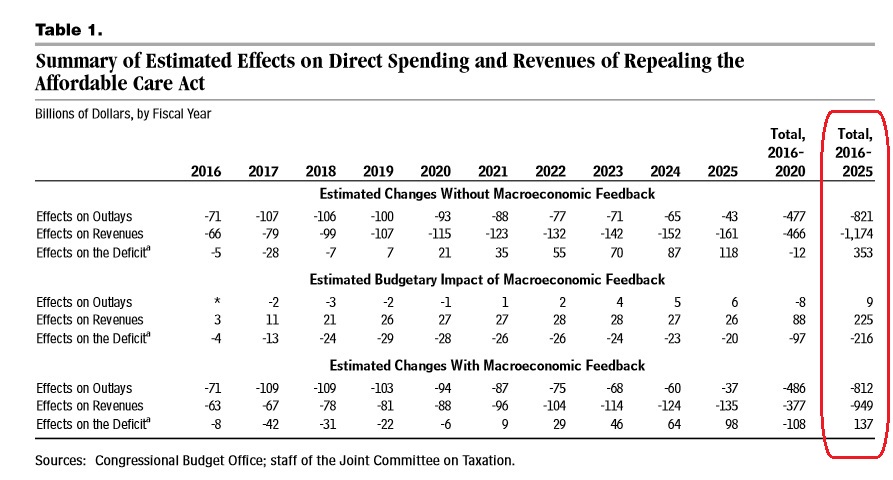
 including a torpedo and an anti-aircraft gun, Der Tagesspiegel website reports. …the army had to be called in with modern-day tanks to haul the Panther from its cellar. It took about 20 soldiers almost nine hours to extract the tank… It seems the tank’s presence wasn’t much of a secret locally. Several German media reports mention that residents had seen the man driving it around town about 30 years ago. “He was chugging around in it during the snow catastrophe in 1978,” Mayor Alexander Orth was quoted as saying.
including a torpedo and an anti-aircraft gun, Der Tagesspiegel website reports. …the army had to be called in with modern-day tanks to haul the Panther from its cellar. It took about 20 soldiers almost nine hours to extract the tank… It seems the tank’s presence wasn’t much of a secret locally. Several German media reports mention that residents had seen the man driving it around town about 30 years ago. “He was chugging around in it during the snow catastrophe in 1978,” Mayor Alexander Orth was quoted as saying.